“An interesting debate has started within the UK MSology community. Do DMTs that have been shown to reduce relapses, relapse associated disability progression, MRI inflammatory activity (focal lesions), MRI associated damage (T1 blackholes and brain volume loss) delay the onset of SPMS? Some of us want class-1 randomised controlled, double-blind, data to show this before we accept that DMTs may delay the onset of SPMS.”
“I think this argument is superfluous, SPMS is a academic construct to explain a clinical phenotype and is not backed by biology. Most of us accept that the pathological substrates that underpin progressive MS are demyelination, neuroaxonal loss and gliosis, which when combined with a failure of neuronal reserve manifests as progressive MS clinically. If we accept a biological definition of progression then progressive MS is present from the start of the disease, in fact it probably starts before you present with your first clinical attack or symptoms. New data shows that RISers (people with radiologically-isolated or asymptomatic MS) already have brain atrophy. In my opinion, any treatment that reduces or prevents these pathological mechanisms that drive progression will delay the onset of clinically-defined SPMS.”
“The problem with our clinical definitions is that they are so unreliable and are a moving target. In the pre-DMT era SPMS used to be diagnosed when MSers had EDSS scores of 2.0-2.5. Now that we have DMTs most people will only diagnose SPMS when MSers are more disabled with EDSS scores above 4.0. Why? Simply because funders will only pay for DMTs in MSers who have relapsing disease. As soon you label someone with SPMS it makes it difficult to prescribe DMTs. How can we rely on a clinical definition of SPMS, when we are continuously changing the definition?”
“I have sat on countless steering committees that have tried to operationalise time to onset of SPMS as a clinical outcome. It has not been possible to reach any consensus. Most of us are now trying to use EDSS milestones instead, for example time to confirmed disability progression to EDSS 4.0. Why 4.0? Most natural history studies suggest that once MSers hit 4.0 the disease progresses relentlessly regardless of whether or not they have superimposed relapses or not. I am not sure if this is correct. Most of our observations are based on natural history studies and not what happens on DMTs. A lot of new emerging data suggests that things are very different in the DMT era; we cannot rely on natural history data to make decisions about the onset of SPMS. For one we need to consider the concept of the therapeutic lag; this based on the hypothesis that in MSers with reduced reserve capacity, disease progression occurring now has been primed by inflammation from one to two years ago. If you switch off inflammation now you need to wait three to five years to see an impact.”

“The other problem I have is that our definition of SPMS tends to be defined by lower limb motor activity. What about the other neurological systems? This is why I think we need to seriously rethink our definition of what is progressive MS.”

There is little doubt in my mind that if DMTs reduce end-organ damage they will delay disability progression and delay the clinical onset of SPMS, however, you want to define it. At a recent Charcot meeting there was a very eloquent presentation by Maria Trojano, who reviewed all the real-life data sets on the impact of DMTs and the course of MS; apart from the British Columbia register all the other data sets showed that DMTs delayed the onset of clinically-defined SPMS. The issue for purists is that this data is not collected in randomised trials and is therefore unacceptable. What do they want?”

“This debate reminds me of what happened in the rheumatology field 15 years ago. When I did my PhD I worked in Marc Feldmann’s and Tini Maini’s laboratory; this duo pioneered the clincal development of anti-TNF (tumour necrosis factor alpha) therapy in rheumatoid arthritis. Anti-TNF therapy switched off the inflammation and made RAers feel well. This triggered a debate whether or not this would prevent end-organ joint damage and the need for joint replacement therapy in the future. Marc Feldmann had no doubt about the longterm impact of these therapies. Why? He understood the biology of RA and knew that inflammation was the driver of end-organ damage; switch it off and you protect joints. Marc has now been proved correct; it is clear that the number of joint replacements required in RAers has plummeted. Maybe we should start counting walking sticks and wheelchair numbers? We already do; EDSS 6.0 and 7.0 are measured surrogates for sticks and chairs. If DMTs are reducing time to EDSS 6.0 and 7.0 they are reducing the needs for sticks and chairs. If the clinical onset of SPMS is linked to EDSS progression then DMTs are delaying the onset of SPMS.”
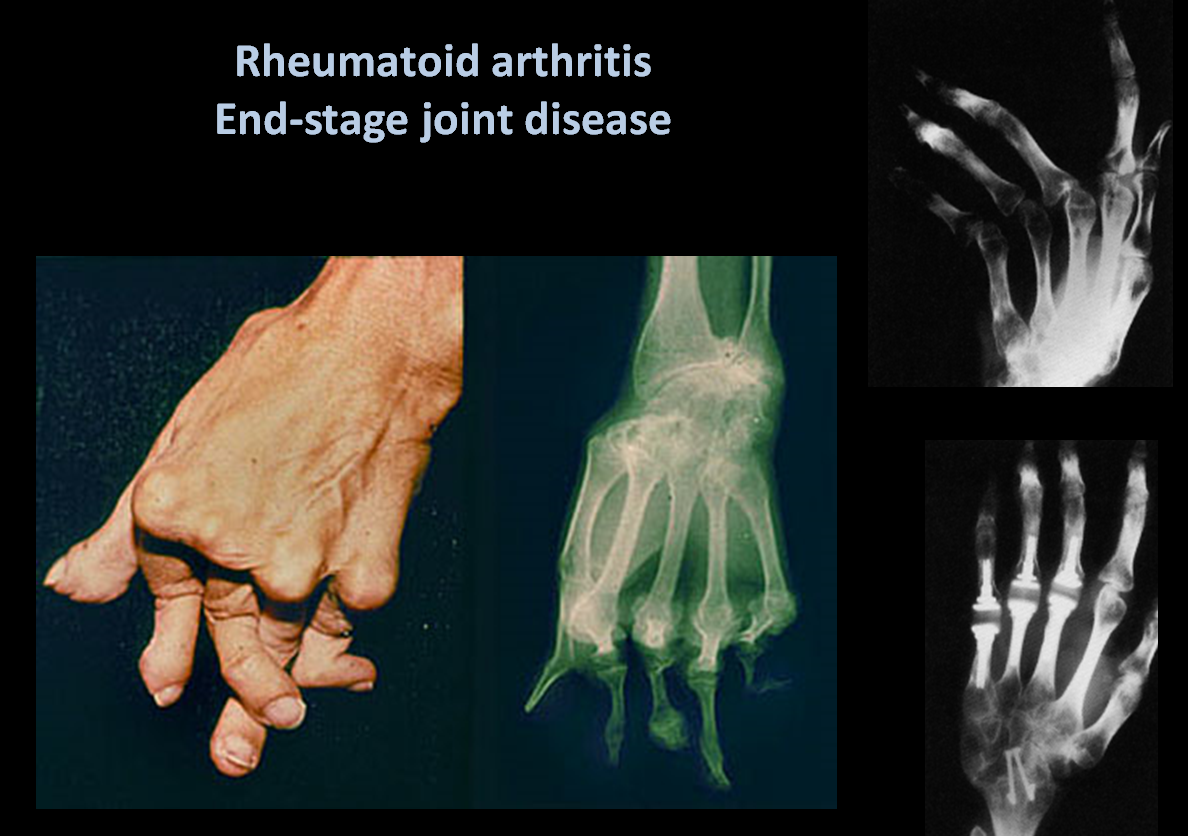
“Unfortunately, unlike joint replacement therapies in RA, or renal dialysis, or transplantation in other end-stage organ failures, we can’t replace the brain and spinal cord, nor can we restore their function when they fail. It is time to think of DMTs as preventive therapies; prevention of disability. We shouldn’t get too bogged down in how we define this; particularly clinically. We need to remember the iceberg analogy.”

CoI: multiple
British neurologists make me sick; what planet do they live on? Do they know that they have a responsibility to look after their patients?
Prof G, thank you for fighting our corner. Hopefully, you will change the naysayers minds about DMTs.
Again, you give us hope. Reading comments elsewhere about the effectiveness or otherwise of DMTs can make you feel in despair: it's good to know your conclusions. From an MSer on first-line therapy.
"The issue for purists is that this data is not collected in randomised trials and is therefore unacceptable. What do they want?"Are they expecting to run 15 year placebo controlled trials so that they can determine if DMT's prevent SPMS? I think this is impossible to do not to mention unethical. I guess this is a way for people who have no clue about what drives ms a way out instead of trying to understand the disease.It is clear that when demyelination ocurrs, the axons undergo a profound change that is going to lead to axonal death due to mitochondrial dysfunction. Theses changes also appear in remyelnated axons for which apear to be NAWM on MRI scans. So looking at the mechanisms that create progression in MS, DMD's will prevent disability if they are started early enough in the disease.
Re: "Are they expecting to run 15 year placebo controlled trials?"Yes, some of my colleagues would like placebo-controlled trials to answer this question. The problem is you wouldn't be able to recruit for such a trial, which is why the debate is moot. Therefore we have to fall back on other indirect evidence, for example what happens to MSers on treatment in real life.
Prof G,I had first infusion of Alemtuzumab five years ago. I'm NEDA on the basis of annual MRIs, stable annual EDSS and no relapses. My EDSS is 3.5. What is my MS category (I was highly active RRMS when I joined the trial)? Also, is any research team looking at treatment to reduce EDSS scores?
In answer to your second question- Yes
To the first question…Responding well…long may it continue
I have been thinking about something that Dr. Dre said a few weeks ago where he argued that Big Pharma ought to compensate MSers who develop SPMS despite being on 'bells and whistles' new DMTs.Dre is right. The costs and the risks of new DMTs are huge, and we need protection. No-one is thinking about us; they're just trying to force through an agenda. If I was to develop SPMS after my treatment with Lemtrada then my disability costs should be provided for by those profiteering from false information. We need a contingency strategy.
Have pharma ever provided information that it Lemtrada will stop SPMS developing?I Don't think they have
MouseDoc, you're whole mantra is based around new DMTs preventing disability. That is false advertising.
I agree; I don't think there is any data that out there that shows that alemtuzumab prevents SPMS. At the moment it is hypothesis that is being tested. What Genzyme need to do is commit to at least 20 years of follow-up to see what happens.
I'm so glad that DMTs were not available when I was diagnosed. I was quite ignorant and believed my life would be in a wheelchair unable to feed myself. I was completely wrong I have managed quite well and now have SPMS. I really do not know how I would have managed to make the difficult decision whether to go onto DMTs.
The image of that shrunken MS brain above a destroyed RA joint scares me.
Excellent post. Is there anything that can be done to change your colleagues minds about this very important issue?
As noted above, I'm not quite sure why you keep putting up the photo of the shrunken brain. I know this disease is bad – I live with it every day. This blog has reached a point hereby one message is king – "MS is a bad disease which will destroy most aspects of your life (relationships, career, mobility etc.), to stand any chance you need to get one of the highly effective treatments as soon as possible after the first sign of the disease (although this is just a hypothesis which will require 20 years to test)"I'd like a few more stories for those who won't benefit from early highly effective treatments e.g. Stem cell research and trials, remyelination research and trials, neurorestoration research and trials, results from treatments for progressive MS…. I think I saw on the MS Society website that Prof M has been given a big grant to look at stem cells. Any news on the progress being made?I love this blog and am grateful for all your efforts, but I don't want it to become a one trick pony ie just early highly effective treatment
I second the sentiments expressed above – positive news can be very reasurring and a relief from anxiety which in turn can soothe symptoms.
We are reporting on what is being published. When the repair studies report we can comment.
I find these posts both helpful and frightening .My MS is 'not too bad', could even be classed as benign, except that it isn't anymore and I just do not know how to shake up my neurology team into being more proactive. Treating my MS instead of mopping up the damage in years to come. Obviously treatment may not work, but the nihilism and complacency is paralysing!
Unfortunately, most MSers with benign MS turn out not to have benign MS. The aim of treatment is to make sure all MSers turn-out to have benign MS.
The onset of my MS was followed by a period of relapses some so bad I was hospitalised. I became ill and was an inpatient at a different large teaching hospital. It turned out to be an MS attack. A couple of years later my new neurologist said I had benign MS. I'd never heard of this term before. So how does a neurologist define "benign MS"? What is it?
If the biology of MS does not differentiate between RRMS, SPMS and PPMS then maybe the labels should be dismissed. A patient has MS period. Let the pathology dictate the treatment not the label.
RE; " Let the pathology dictate the treatment not the label."Yes, I would agree with this. The problem is most neurologists think they can predict the pathology from the clinical phenotype. Do don't want to admit how unreliable the clinical phenotype is. What we need is a reassessment of how we classify MS so that we can treat it better. If we did PPMSers may not feel that hard done by.
But, unless i'm wrong, there is still no treatment for PPMS. Renaming is the equivalent of moving the deckchairs on the Titanic. The issue is much simpler – stop the disease and repair the damage. Renaming phenotypes, coming up with scales to assess the severity of the multitude of symptoms doesn't help MSers. So much can learned from the cancer sector. You guys limit yourselves at the outset by looking for treatments to slow down progression by tinkering with the immune system. Why can't the world of MS research tell me what's causing the destruction of my brain tissue? It's a simple question, but there's never an answer!
I'm a PPMSer. Please rename my phenotype and then tell me what treatment I can have (my current neuro tells me there is nothing for my condition).
I know of many PPMSers who have had progression stopped with HSCT.Some are progression free over 3 years.
EDS scores do little to measure neurological damage and in my experience little evaluation of neurological damage is undertaken on a routine basis by neurologists. Much easier to record changes in physical functioning.