It has been ~5 years since I approached Genzyme with a hypothesis to derisk alemtuzumab. I first posted on the topic of derisking alemtuzumab on the blog in 2014. I discussed derisking infusion reactions and secondary autoimmunity.
The immune system has many mechanisms in place to prevent autoimmunity. When you learn how the immune system works it is really quite surprising that autoimmunity is so uncommon. What the immunologists tell us is that there must be a series of underlying biological processes that are causing secondary autoimmunity and if we can work out what these are we can intervene and prevent this complication. This is what the Professor Alasdair Coles, and Dr Joanne Jones, have been trying to do in Cambridge. They think that because the immune system reboots itself from peripheral memory cells it is more likely to result in an aberrant autoimmune responses. They have done a trial to encourage rebooting of the immune system using more naïve cells from the thymus. They have treated MSers after alemtuzumab with a hormone called, Palifermin, that stimulates the thymus to produce more naïve T-cells. The study is called the Cam-Thy study.
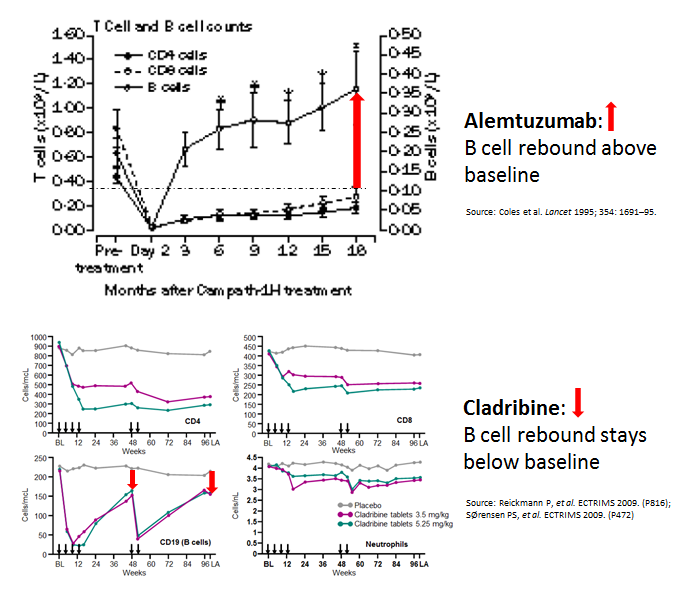
We have a different take on what is responsible for the secondary autoimmunity and wanted to test a different strategy; we hypothesised several years ago that it was due to B-cell hyperproliferation. Based on our hypothesis Palifermin should exacerbate the problem; increasing reconstitution with naive cells without regulation will increase secondary autoimmunity.
In response to the challenge above the Mouse Doctor and DrK have analysed the alemtuzumab reconstitution data in more detail and the analysis strongly supports this hypothesis. Where to from here? I think we could still do a proof-of-concept trial, but focusing on anti-drug antibodies, i.e. anti-alemtuzumab antibodies as the readout. Alemtuzumab is a humanised antibody and the incidence of anti-drug antibodies should be very low. Alemtuzumab appears to break immune tolerance and the mechanisms that underlie anti-drug antibodies may be the same as those that underlie secondary autoimmunity.
Baker et al. Interpreting Lymphocyte Reconstitution Data From the Pivotal Phase 3 Trials of Alemtuzumab. JAMA Neurol. 2017 Jun 12. doi: 10.1001/jamaneurol.2017.0676.
IMPORTANCE: Alemtuzumab, a CD52-depleting monoclonal antibody, effectively inhibits relapsing multiple sclerosis (MS) but is associated with a high incidence of secondary B-cell autoimmunities that limit use. These effects may be avoided through control of B-cell hyperproliferation.
OBJECTIVE: To investigate whether the data describing the effect of alemtuzumab on lymphocyte subsets collected during the phase 3 trial program reveal mechanisms explaining efficacy and the risk for secondary autoimmunity with treatment of MS.
DESIGN, SETTING, AND PARTICIPANTS: Lymphocyte reconstitution data from regulatory submissions of the pivotal Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis I and II (CARE-MS I and II) trials were obtained from the European Medicines Agency via Freedom of Information requests. Data used in this study were reported from June 22 to October 12, 2016.


>You get similar efficacy from ocrelizumabThis hasn't ever been proven.
Isn't it interesting how one can claim (in the same breath) Ocrelizumab to have good NEDA rates and no information re atrophy lol.
Brain atrophy is NEDA-4 classical NEDA does not include this measure
lol but if the ms brain shrinks faster then normal brain AND this faster shrinking is part of the cause of irreversible disability, then the fact that your fine print excludes atrophy from NEDA does not change that NEDA in this case is completely misleading.The issue being, when the fine print is too fine, things like misleading and deceptive conduct arise (I think you have the same in the UK)…. and in this case, in my view, the concept of neda is misleading and deceptive 🙂
NEDA is a good as for what you look at, it will evolve we should be using NEDA-5 at least, as a lawyer you know the detail is in the fine print.NEDA has to be the aspiration for treatment. How this is monitored is key, seems like blood neurofilament should be one.
lol by definition you can't have 5 levels of "no evidence of disease activity". if there is no evidence then there is no evidence, it can't be that we have 5 steps of evidence or five types of evidence. (then it's not "NO evidence of disease activity" – then it is "no evidence of symptoms XYZ – which we hand picked to include (rather than which point to no evidence of disease activity).say you have a cold. and someone devises a neda approach. How can it be thatNEDA 1 = no evidence of disease activity 1 because the person is not sneezingNEDA 2 = no evidence of disease activity 2 because the person neither sneezing nor coughing.NEDA 3 = no evidence of disease activity 3 because the person is not sneezing, coughing or has a blocked nose. NEDA 4 = no evidence of disease activity 4 because the person is not sneezing, coughing, has no blocked nose and is not fatigued.Surely you see that all 4 simple cannot be NEDAs? Sneezing is not a NEDA measure of a cold if you are ignoring the other 4 symptoms lol. Then we are not aspiring or measuring NEDA, we are just using pretty feel good names to pick and choose which symptoms or measures of evidence of disease activity we use.You haven't changed what you are doing you have changed what you are calling it
Looks like the Camthy study has struggled a bit. It has taken them 5 years to recruit 86 patients… Is this because it was wishful thinking in the first place or am I being naive about how rare alem. use is.? Your new paper is really interesting, not sure about the feasibility, for the reasons you have given I am not sure it will get commercial/clinical buy in….
It's been terminated according to Prof Coles' blog but is the £900,000 + study is still down as being active.
Sounds traumatic.
Prof Coles should publish the result
Indeed, if the result is as I suspect, it might be illuminating about the immunology of MS.
Given all three options, I'd still choose Alemtuzumab. There's a suspicious silence in the lack of brain atrophy data with Ocrelizamub. And the NEDA rates in the Alemtuzumab trial was still better than those in the cladribine trial.
Please read Rotstein et al are you looking at the phase II and not the phase III where NEDA rates were much most disappointing.
I'm sorry, this reply confuses me?
Evaluation of no evidence of disease activity in a 7-year longitudinal multiple sclerosis cohort. Rotstein DL, Healy BC, Malik MT, Chitnis T, Weiner HL. JAMA Neurol. 2015 Feb;72(2):152-8. doi: 10.1001/jamaneurol.2014.3537Alemtuzumab MS-CARE- 1 NEDA 39%Alemtuzumab MS-CARE- 2 NEDA 32%Cladribine CLARITY NEDA 46%The effect of alemtuzumab was much more impressive in the phase II trial compared to the phase III trial.
How many years does that cladribine NEDA include? Those Alemtuzumab NEDA values are for two years post treatment, not 7.Prof G can you please elaborate on the cladribine figure here, I'm pretty sure Alemtuzumab fared better than cladribine in the trials.
both are 2 year trial data.The CLARITY extension study is I think being written up.
Nice post At waht time point will you take rituximab ? To avoid b cell overshooting?Thanks Luis
I would think around 1-3 month,
MouseDoctorWednesday, June 21, 2017 12:39:00 amBut what if ocrelizumab is a PIRT/Induction therapy.lol for as long as neuros and payers reckon that it's not (current state of affairs), the fact that it may become that sometime in the future (when – 2 years? 3 years? 5 years? 10 years?) doesn't really help those getting infused every 6 months for what is right now and indeterminate amount of time.Of course, if it comes out in 5 years time that they've been overdosing a whole bunch of ms patients while the data was available to suggest otherwise, neuros will say ooops we didn't know.
Once the serious infection issues start to arrive, maybe their mind will be focusedThe data is available, nowhttp://www.ebiomedicine.com/action/showFullTextImages?pii=S2352-3964%2817%2930045-2
I have this theory that neuros are still playing at being doctors. If the earliest DMTs arrived about early 2000s on a popular setting, then it seems to my uncharitable eye, they didn't really have much to offer before that (must depressing and soul destroying). If they refer out many of their patients' symptoms (urinary, physical therapy, pain management etc) – then other than the EDSS testing, they didn't really have much doctorial things to do. As the patients weren't on DMTs they didn't really have that many side effects to deal with that they couldn't simply refer out.In the last 15 years not only do they have patients and drugs to prescribe, but also side effects to boot – cept they are just learning.Someone's comment on this blog made me have that revelation lol
I would also still choose alemtuzumab based on the current evidence. My reading of the clinical research suggests that it has a small, but significant advantage over ocrelizumab. The real difference for me between these two drugs has to do with their long-term safety. I prefer rolling with the dice with the three serious, but treatable auto-immune conditions that may come with alemtuzumab than the unknown risks that ocrelizumab may pose in the long-term in terms of opportunistic infections and malignancies. How safe is it to deplete your B cells every six months?
How safe is it to deplete your B cells every six months?Isn't that what rituximab does ? and it seems safe.
But there have been opportunistic infections in RA patients being treated with rituximab, including six cases of PML: http://ard.bmj.com/content/early/2012/11/06/annrheumdis-2012-201956.full My point is that we don't have any long-term data on the safety of ocrelizumab.
Sebastian – agreed entirely. We know more about Alemtuzumab due to its long term use in oncology. Plus the brain atrophy data looks good. I'm yet to see any brain atrophy data for Ocrelizumab, let alone any positive data. Adam – yes Rituximab/ Ocrelizamub's target is primarily b-cells. Seems safe? Based on trial results in the short term, but I suspect malignancies take time to develop and present. At least with Alemtuzumab the body has the opportunity to rebuild a competent immune system without being disrupted every 6 months.
But what if ocrelizumab is a PIRT/Induction therapy.See our B cell paper with the phase II extension data
Did the Cambridge trial make autoimmunity more likely then? I've always been put off alemtuzumab by the thyroid issue despite the fact I'd love to take an induction treatment. Are you going to put together a proposal to trial your idea?
The autoimmunity issue is notably a problem in MS. When alemtuzumab used in cancer this is not a notably issue, suggesting MS genetics gives a predisposition.Are you putting a proposal to trial…..we did about 5 years ago.However I could suggest another one.
Jims- is be far less concerned about thyroid autoimmunity than I would about the other more serious, albeit rarer, autoimmune diseases.
I have to agree with previous post, as of today, with the evidence we got in hand… I would still go for alemtuzumab, and have HSCT as the backup plan… They need to show me brain atrophy data that beats alemtuzumab, every year report seems to get even better… Yes there's risk and its disheartening that more hasn't been done to prevent secondary effects.
One thing to keep in mind is the speed at which these secondary effects appear with alemtuzumab. I got ITP 5 days after a 'normal' blood test result (they'd been perfect for 2 years). My platelets dropped from 173 to 3 in that time. Luckily I noticed the rash and acted. I'm concerned that the monthly bloods aren't enough on their own and that even an engaged patient might not pick it up before they bump their head. When you're getting on with life it's easy to forget No harm done and am on the road to recovery with first line treatment (prednisone). Am still happy with alemtuzumab as a treatment – just worried like it's a matter of time before the holes in the Swiss cheese line up. 'Within the normal range' might need to be baselines for the individual with some consideration for trends
Cyril, thanks for this reminder to be vigilant. I understand we can get urine test strips to monitor the kidneys between the monthly tests. Pity they don't have something the patient can do at home for platelets!
Cyril,I hope your experience with Alemtuzumab is as good as mine – first infusion 11 years ago and second infusion 10 years ago. Since first infusion – no relapses, no activity on MRI, stable EDSS (some improvement after first infusion). I've just come in from mowing the lawn (large garden) and then lugging in a new sofa which my wife ordered (and didn't tell me about). I did get Graves disease which now requires a tiny thyroxine tablet once a day. My neuro team at Cambridge have been brilliant – monitoring, responding quickly to queries / concerns. Was the choice of Alemtuzumab difficult. No – had highly aggressive RRMS ( attacks left me bedbound for a couple of weeks); had small children; do not have the sort of personality to deal with wheelchairs, worsening disability. There are risks of secondary autoimmune diseases, but risks can be mitigated by good monitoring + the recipient taking on their own monitoring and alerting the neurology team. My two kids will soon be heading to Uni. I've never discussed MS with them. All they know is that dad's knee / ankle gets a bit stiff after walking for 45 mins. Would I do the same thing again? Yes. I have a stack of annual holiday photos on beaches with the family etc. I wouldn't have had them without Alemuzumab.
LGO – a home platelet test would be very handy! I have a stack of blood test forms now separate to bloodwatch that I will be using on suspicion in future. For some reason my team was a little reticent to use one of the 'spare' bloodwatch when I first suspected something was happening. I don't think they'll be hesitate next time though :)Anon – I hope so too! Thanks for relaying your experience. It has been very effective for me too so far, and has enabled so much of my life to move forward.
Currently I am fascinated with the Henry Martini rifle; the 'Zulu rifle'. Technologically this rifle bridged between black powder vs smokeless, breach vs muzzle loaders and cartridges vs bullet&charge. It is interesting that this bridging technology required workarounds to make it work. The cartridge had a paper cone to help clean the barrel. I think that alemuzumab is a bridging technology.