Why should you die earlier because you live in the North of England? #ClinicSpeak #ResearchSpeak
As I get older I seem to be getting more political, more outraged and more upset by healthcare inequality. I posted on this topic last month. The paper below that has just been published, and was allover the news yesterday, demonstrates a country of two tales. If you live in the North of England you are destined to die prematurely. The paper concludes with the statement:
“This profound and worsening structural inequality requires more equitable economic, social and health policies, including potential reactions to the England-wide loss of improvement in premature mortality.”
Why is this relevant to MS? Because it plays out in the MS space as well; please see ‘A Lottery of Treatment and Care’ document below from the MS Society. MS services, access to MS services, poor lifestyle (diet, exercise), comorbidities (other diseases) are only a few examples that are affected by inequality that will also impact on outcomes for people with MS and contribute to the North-South divide.
When I have attended the MS Life meeting in Manchester in the past I would spend 1 or 2 days running an informal MS clinic. Attendees at the Manchester meeting, who tend to be from the North of England, would tell me stories about no, or limited, access to continence advisers, functional electric stimulation, MS nurse specialists, cognitive behavioural and other therapists, DMTs and much, much more. The problems are not because of the services provided by the specialist units in the North – they are excellent – but, it is an institutionalised problem of poor access to these units and low expectations from pwMS and their families.
We as healthcare professionals working in the NHS should be ashamed of ourselves; ashamed to be presiding over such a disparity in health outcomes. I am going to ask Julia Pakpoor, who is a collaborator of ours, to look into mortality of MSers in England. I hypothesise that if you have MS and live in the North of England you are likely to die earlier. I hope I am proved wrong.

Buchan et al. North-South disparities in English mortality 1965–2015: longitudinal population study. J Epidemiol Community Health 2017;71:928–936.
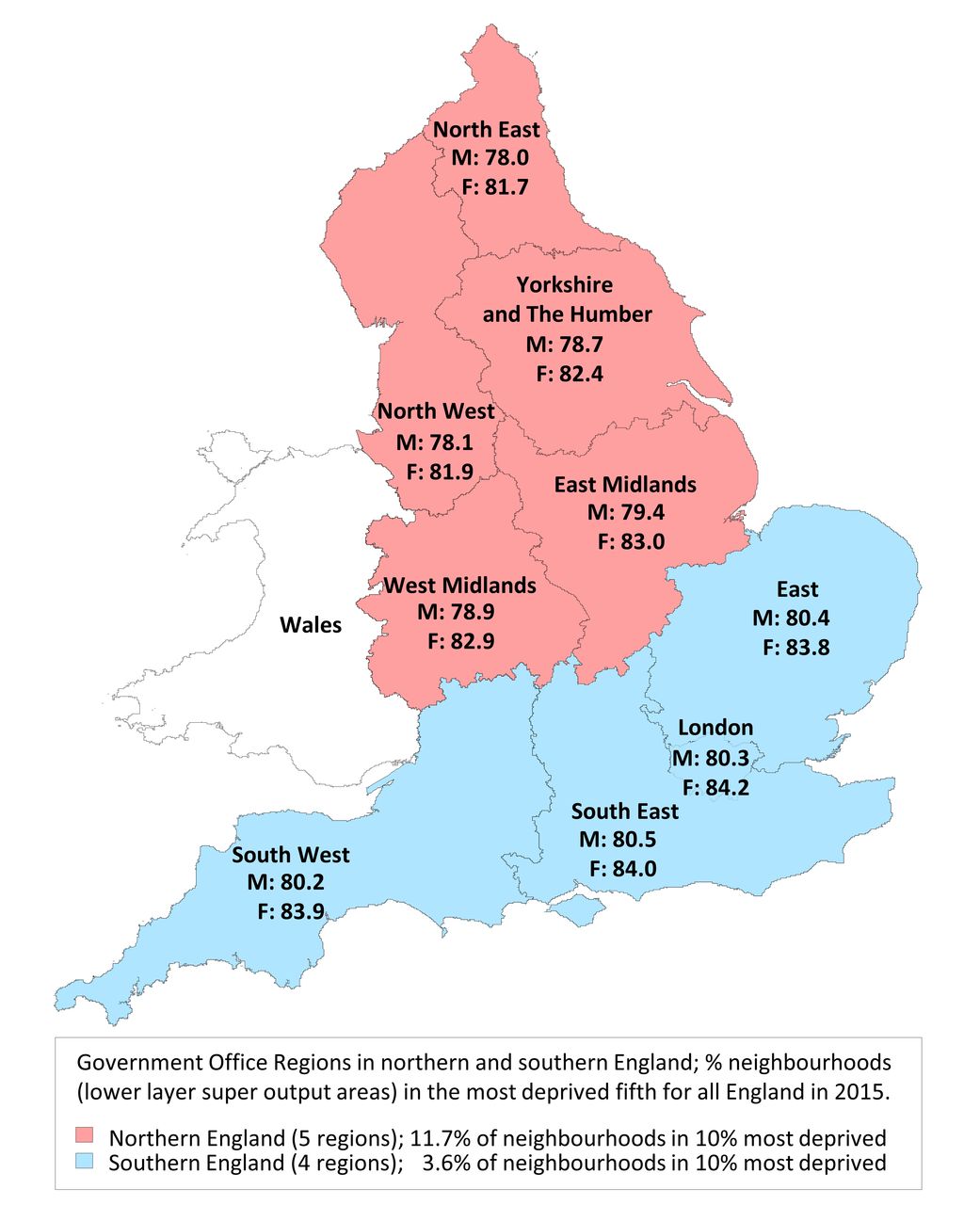
Background: Social, economic and health disparities between northern and southern England have persisted despite Government policies to reduce them. We examine long-term trends in premature mortality in northern and southern England across age groups, and whether mortality patterns changed after the 2008–2009 Great Recession.
Methods: Population-wide longitudinal (1965–2015) study of mortality in England’s five northernmost versus four southernmost Government Office Regions – halves of overall population. Main outcome measure: directly age-sex adjusted mortality rates; northern excess mortality (percentage excess northern vs southern deaths, age-sex adjusted).
Results: From 1965 to 2010, premature mortality (deaths per 10 000 aged <75 years) declined from 64 to 28 in southern versus 72 to 35 in northern England. From 2010 to 2015 the rate of decline in premature mortality plateaued in northern and southern England. For most age groups, northern excess mortality remained consistent from 1965 to 2015. For 25–34 and 35–44 age groups, however, northern excess mortality increased sharply between 1995 and 2015: from 2.2% (95% CI –3.2% to 7.6%) to 29.3% (95% CI 21.0% to 37.6%); and 3.3% (95% CI –1.0% to 7.6%) to 49.4% (95% CI 42.8% to 55.9%), respectively. This was due to northern mortality increasing (ages 25–34) or plateauing (ages 35–44) from the mid-1990s while southern mortality mainly declined.
Conclusions: England’s northern excess mortality has been consistent among those aged <25 and 45+ for the past five decades but risen alarmingly among those aged 25–44 since the mid-90s, long before the Great Recession. This profound and worsening structural inequality requires more equitable economic, social and health policies, including potential reactions to the England-wide loss of improvement in premature mortality.
Stop moaning and start producing some breakthrough research! Average life expectancy in your beloved South Africa is 57 – that's real inequality. I think that's something to worry about more than the reason behind Mrs Smith in Clapham living to 84 and Mrs Smith in Preston living to 82. Pay some voluntary tax if you are that concerned instead of indulging in expensive fine wines! The term Champagne Socialist fits you like a glove – sitting in your suburban garden with a glass of wine worrying about the poor in Tower Hamlets as you write out the cheque for your children's private school fees.
Ouch, the politics of envy. It hasn't help the Venezuelans.
Troll? I would suggest you take down this comment. It very unhelpful and not in the spirit of this blog.
It's okay. I don't mind people having an opinion about my position. It's what this post is about inequality.
Good point about Venezuela; its an example of how socialism has failed the masses and allowed government officials, the police and military to rape and pillage the country. Our colleague from Colombia tell us that the number of Venezuelan refugees crossing the border into Colombia is staggering; a humanitarian disaster that has been man-made.
Nothing wrong with enjoying fine wine and champagne. It's what keeps France's economy going.
I wouldn't be surprised if longevity is associated with champagne & fine wine consumption and attendance at a private school. The latter are associated with wealth and its the wealth that drives outcomes. Prof G based on this you may live beyond 80.
And people, in particular Londoners', wonder why Northerners' voted for Brexit.
Spot on! Until we address inequality the drivers of Brexit will get larger and society will be come more divided.
Until people understand that the problems they are having have little to do with being in the EU? The EU is a convenient scapegoat. Not least for the politicians of the day – allows them to evade finding real answers, the fruit of which will only grow beyond their terms of office. Come on, stop peddling the myth.
At least the EU supports equity of access; to jobs, capital, education, healthcare, etc. Will post-Brexit Britain do the same?
I think you will find that ovet 800,000 Poles have moved to the UK for work and a better life (just using Poles as an example). UK citizens moving the other way probably less than 1,000. It was this sort of inequity which contributed to Brexit. Many Greek civil servants got retirement at 50 with a pension the equivalent of their salary. I would have liked that but some of the UK's contributions bailed out Greece. It was this sort of inequity that led to the vote to Leave.
"I think you will find that…"Anyone who knows anything about history and is being honest knows that is extremely narrow minded and hypocritical. Looking at the history of Scottish emmigration, as one small example: In the 15th, 16th and 17th centuries there was strong colonisation of Poland by Scottish people, there were about 400 small settlements of Scots in Poland and Lithuania. Immigration and emmigration is part of life, human history.
You lucky you don't live in the US. The disparity between the haves and the havenots is even larger.
There are so many factors which explain why there are differences in lifespans across different parts of the UK e.g. levels of obesity, levels of smoking, levels of alcohol consumption, occupation (heavy industry in the north), Vit D levels….. I suspect there is more availability of private healthcare in the south. Some diseases are more prevalent in the north (combo of heavy industry and lower levels of Vit D). However, things will even out as more northerners move south e.g. Prof Mouse = from industrial north, ex- smoker, big drinker, clinically obese. He has moved to London which should in time lower the south's average life expectancy ((Will Rogers effect).
Ha ha, industrial north…far from it
Well done MS Society – leave Shetland off your map entirely – world class hotspot of MS. So in touch, as always.
Have you ever been up North, Prof G? Do you even know how we live? Our worries? Our neglect?
Many times; where do you want me to start Morpeth, Hull, Grimsby, Preston, Blackpool, Sunderland? Or should I stick to the big cities or country villages? My favourite village is Flash (Midlands, but still north of London).
And judging from the little utilized hospital-based ambulatory centers popping up like weeds in a garden, they don’t know either. age defying