Barts-MS rose-tinted-odometer: ★
I know it sounds like a cliche but Catch-22 would definitely be on my list of most impressionable books I read as a teenager. I liked it because of its dark satirical humour, it was written in the third-person and it taught me how absurd war actually is. Catch-22 (and the Great Gatsby) also taught me if you love a book you should never watch the movie; the screenwriters, actors and directors can never do your imaginary characters justice.
The book has become so influential that ‘Catch-22’ has become a noun and refers to a dilemma or difficult circumstance from which there is no escape because of mutually conflicting or dependent conditions.
Although I am meant to be at home recovering from injuries I am doing some emails. Over the last few days, I have received numerous emails from patients and neurologists asking for advice about COVID-19/SARS-CoV-2 vaccines and DMTs and what am I telling my patients. One patient tells me that her neurologist referred her the excellent MS Society webpage for advice, but the site then referred her back to her neurologist for definitive advice. A Catch-22?
Some US neurologists have picked-up that my advice and position on vaccines and vaccine readiness has changed since I first started talking about this issue on the blog. They are correct, my position has changed. I always took the position that we should continue to manage MS the way we managed it before COVID-19 with certain caveats* around the risk of being exposed to SARS-CoV-2 and whether or not individuals could self-isolate or not, and that we should cross the vaccine bridge when it arrives. Now that the vaccines are arriving and the ambitious national roll-out suggests the whole country will be vaccinated within the next 6 months, advice has to be given and given quite quickly.
In my opinion, all the COVID-19 vaccines that the UK Government has purchased can be used in people with MS regardless of whether or not they are on a DMT. This advice is based on the fact that the MHRA and other regulatory bodies have licensed or will license these vaccines because of their safety and efficacy profile in the general population.
Importantly none of these vaccines is likely to be a ‘live viral vaccine’. There is some confusion around the Oxford-AstraZeneca vaccine that does use a chimpanzee adenovirus vector to deliver the immunogen to our cells so that the immunogen can be expressed. The virus in this vaccine is able to infect cells and express its relevant proteins, but because some of its genes for replication have been mutated it cannot replicate itself and cause ongoing infection. I am not sure how this vaccine will be classified by the MHRA or other regulatory authorities, but in my opinion, it is likely to be safe to use in pwMS.
I say these vaccines are likely to be safe in pwMS. However, none of the COVID-19 vaccines has specifically been tested in pwMS so we have to extrapolate data from the general population data. There may be something we don’t know about having MS that predisposes pwMS to some rare complications. However, based on other vaccines that have been used in MS this is very unlikely.
It is clear that being on some immunosuppressive DMTs may reduce your chances of responding adequately to the vaccine and hence being fully immune to infection from wild-type SARS-CoV-2. Until we do detailed immunological studies in pwMS on each DMT we won’t be able to answer specific questions about each DMT with certainty.
Interferon-beta , glatiramer acetate and immune reconstitution therapies
In general being on interferon-beta and glatiramer acetate, immunomodulatory DMTs, are unlikely to interfere with vaccine responses. Similarly, if you have had one of the immune reconstruction therapies, such as alemtuzumab, cladribine, mitoxantrone or HSCT in the past and have reconstituted your peripheral immune system you should respond to the vaccines. If on the other hand, you have not had completely reconstitution of your immune system you may still consider having the vaccine, but the immune response may be blunted. Waiting for immune reconstitution or having the vaccine now will be a trade-off between wanting to protect yourself now or waiting months when the pandemic may be almost over. Please note vaccination is not only about you, but slowing and preventing transmission of the virus in the general population, which is a factor you may want to consider. This may relevant, for example, if you want to see unvaccinated vulnerable relatives or if you want to travel to parts of the world with a delayed vaccination programme.
Fumarates, teriflumide and natalizumab
If you are fumarates (DMF, diroximel fumarate), teriflunomide or natalizumab, based on other vaccine studies, COVID-19 vaccine responses are likely to be reasonably preserved. Therefore there is no need to stop these DMTs or delay getting a vaccine if you are on these treatments.
S1P modulators
For the so-called S1P modulators (fingolimod, siponimod, ozanimod and ponesimod) vaccine responses are likely to be blunted, but whether or not the blunted responses will be sufficient to prevent SARS-CoV-2 infection is a moot point. However, I would not recommend stopping these treatments to have a vaccine as these therapies are associated with MS rebound activity. My advice would be that if you are on these therapies to go ahead with the vaccine when it is offered to you.
Anti-CD20 therapies
When I initially wrote about vaccine hesitancy I suggested that pwMS on an anti-CD20 therapy (rituximab, ocrelizumab, ofatumumab) may have to delay their next infusion or miss one or two infusions to allow B-cell reconstitution before they have a coronavirus vaccine. Since making this statement more immunological data has emerged and there really is no definitive evidence to support this position.
Yes, I agree that in general people on anti-CD20 therapies have blunted antibody responses to wild-type SARS-CoV-2 infection and to other vaccines including vaccines with containing new antigens that the immune system has not seen before. However, this doesn’t mean these people haven’t developed immunity to the infection or vaccine that is long-lasting. For one the vast majority of pwMS on an anti-CD20 therapy who get COVID-19 make an uneventful recovery. Why? Almost certainly this recovery is due to cellular and not humoral (antibody) immunity and this immunity won’t vanish and is likely to persist longterm.
Even normal people who have had COVID-19 and who lose their antibody responses still have detectable cellular immunity. My interpretation of this data is that pwMS who are on an anti-CD20 therapy should simply go ahead and have the coronavirus vaccine when it is offered to them and not to worry about whether or not they mount an antibody response.
I am aware that some pwMS are planning to delay their next infusion regardless of what I or their HCP says. The question I ask is for how long? One, two, three or more months? Some pwMS plan to wait for peripheral B-cell reconstitution that can take months to years to occur and even then there is no consensus of what normal B-cell reconstitution looks like. You need to weigh the lack of evidence that delaying your next anti-CD20 therapy or waiting for B-cell reconstitution will make any difference to your vaccine response against the time-sensitive nature of the vaccine to protect you during the high-risk period of the pandemic. If you wait too long and the pandemic is over the benefits of the vaccine will be reduced.
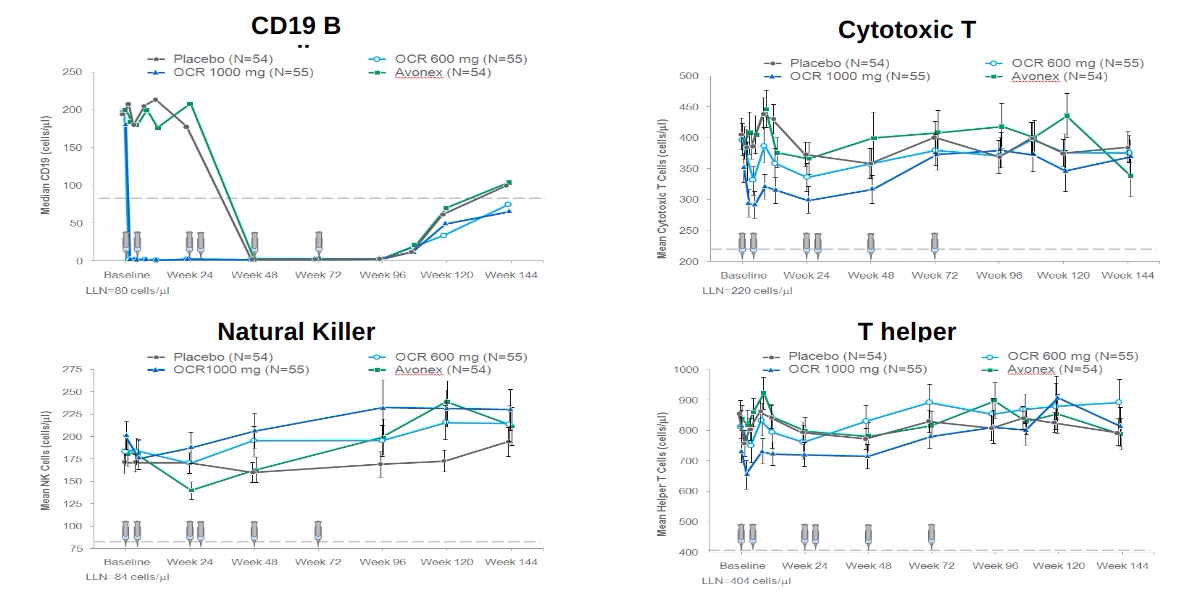
The only evidence base we have at the moment is the recently published VELOCE study that delayed vaccination until 12 weeks after an initial course of ocrelizumab. This study showed blunted, but not absent, antibody responses to recall and new vaccines. Based on this study if you have just had a recent course of ocrelizumab you may want to delay getting the COVID-19 vaccine for 12 weeks after the last infusion. However, as 12 weeks is a long time to wait in the current climate I have been recommending at least 4 weeks; a pragmatic compromise.
In my opinion, it is more important for pwMS on anti-CD20 therapies to be vaccinated than to not be vaccinated. This is because vaccination policy is really about population, or subpopulation, health and stopping the spread of the virus and protecting the individual is a secondary aim.
MS relapses
Will the COVID-19 vaccines trigger MS relapses? This hypothesis is based on extrapolating data on two non-peer-reviewed cases of CNS demyelination in the Oxford-AstraZenca (Ox-AZ) trial and several cases of transverse myelitis in patients who have had COVID-19. One case on in the Ox-AZ trial, who received the vaccine, had an initial attack or relapse and was subsequently diagnosed as having MS; i.e. I assume because they had pre-existing lesions and were now shown to have a second attack or new lesions consistent with dissemination in time. The other case had an episode of vaccine-related transverse myelitis (TM), which is relatively common with vaccines in general. Please note that vaccine-related TM is not MS. The only vaccine that has been reported to potentially trigger MS relapse is the live yellow-fever vaccine and this is based on one report that has subsequently not been replicated. Therefore, there is no current evidence that coronavirus infection or coronavirus vaccines trigger MS relapses. In my opinion, there is no reason to avoid the COVID-19 vaccine based on this hypothesis. Clearly, my opinion may change if new data emerges to the contrary.
Summary
If you have not had COVID-19 having a vaccine will offer you the opportunity of preventing getting COVID-19 or at least if you do get it, of having milder disease. All the licensed vaccines, which have been shown to be safe in the general population are likely to be safe in pwMS. Although some people on immunosuppressive therapies, in particular, S1P modulators and anti-CD20 therapies, may have blunted antibody vaccine responses these may still be sufficient to protect you against infection or at least severe COVID-19. There is no evidence that stopping or delaying treatment, in the hope of boosting vaccine responses will work and may result in you missing out on being protected when your risk of infection is highest. Please be aware that stopping some DMTs, in particular, natalizumab and S1P modulators, is associated with a rebound of disease activity and is not recommended. Hopefully, the pharmaceutical industry and the wider MS community will collect data and do specific studies to answer the many questions we have around vaccination and vaccine responses in pwMS on specific DMTs.
* The caveats refer to alemtuzumab and HSCT, which affect both innate (monocytes and/or neutrophils) and adaptive (particularly cytotoxic CD8+ T lymphocytes), which are required for fighting SARS-CoV-2. My advice for the other DMTs has not to self-isolate, but to simply stick to the current government guidelines in relation to social distancing and personal hygiene.
Bar-Or et al. Effect of ocrelizumab on vaccine responses in patients with multiple sclerosis: The VELOCE study. Neurology October 06, 2020; 95 (14)
Objective: The phase IIIb VELOCE study (NCT02545868) assessed responses to selected vaccines in ocrelizumab (OCR)-treated patients with relapsing multiple sclerosis.
Methods: Patients were randomized 2:1 into Group OCR (n=68; OCR 600mg); or Control (n=34;interferon-β or no disease-modifying therapy). All received tetanus toxoid (TT)-containing vaccine, Pneumovax® (23-PPV) and keyhole limpet hemocyanin (KLH). Group OCR was subdivided into OCR1 (n=33) and OCR2 (n=35) at randomization. OCR1 received Prevnar® (13-PCV) 4 weeks after 23-PPV; OCR2 and Control received influenza vaccine. Vaccinations started 12 weeks after OCR initiation (Group OCR) or on Day 1 (Control).
Results: Positive response rate to TT vaccine at 8 weeks was 23.9% in OCR vs 54.5% in Control. Positive response rate to ≥5 serotypes in 23-PPV at 4 weeks was 71.6% in OCR and 100% in Control. Prevnar® did not enhance response to pneumococcal serotypes in common with Pneumovax®. Humoral response to KLH was decreased in OCR vs Control. Seroprotection rates at 4 weeks against five influenza strains ranged from 55.6–80.0% in OCR2 and 75.0–97.0% in Control.
Conclusion: Peripherally B-cell depleted OCR recipients mounted attenuated humoral responses to clinically relevant vaccines and the neoantigen, KLH, suggesting use of standard non-live vaccines while on OCR treatment remains a consideration. For seasonal influenza vaccines, it is recommended to vaccinate patients on OCR, as a potentially protective humoral response, even if attenuated, can be expected. Classification of evidence This study provides Class II evidence confirming that the humoral response to non-live vaccines in patients with RMS following ocrelizumab treatment is attenuated compared with untreated or interferon-β–treated patients, though can still be expected to be protective.
Twitter: @gavinGiovannoni Medium: @gavin_24211