Summary: This post explains therapeutic lag and why people with more advanced MS don’t see an immediate response to DMTs.
I have been invited to give a grand round talk at Imperial College this morning. I have chosen the topic: “Is progressive MS (more advanced MS) modifiable?”. This is an extension of our #ThinkHand campaign to get the wider neurological community to accept that MS is potentially modifiable throughout its course. Despite us posting and reposting about reserve capacity, therapeutic lag, MS being a length-dependent axonopathy and the asynchronous progressive MS hypothesis we still get questions such as: “Why don’t pwPPMS, or pwMS with an EDSS >6.0 respond, to HSCT and other DMTs?”
It is the same issue in relation to responders vs. non-responders to ocrelizumab in the PPMS trial. It is very difficult to know who is a responder and non-responder based on the current data from the ocrelizumab PPMS, or ORATORIO, trial. Why? Simply because clinical trials are designed, or powered, to get a significant read-out in a reasonable period of time. It doesn’t mean that if someone with PPMS does not stabilise, on a high-efficacy therapy, in say a period of 2 years is a non-responder. Because of therapeutic lag, it may take much longer to see a response to treatment, particularly in pwMS who are older and have less reserve capacity in the particular pathway (usually the legs) being assessed.
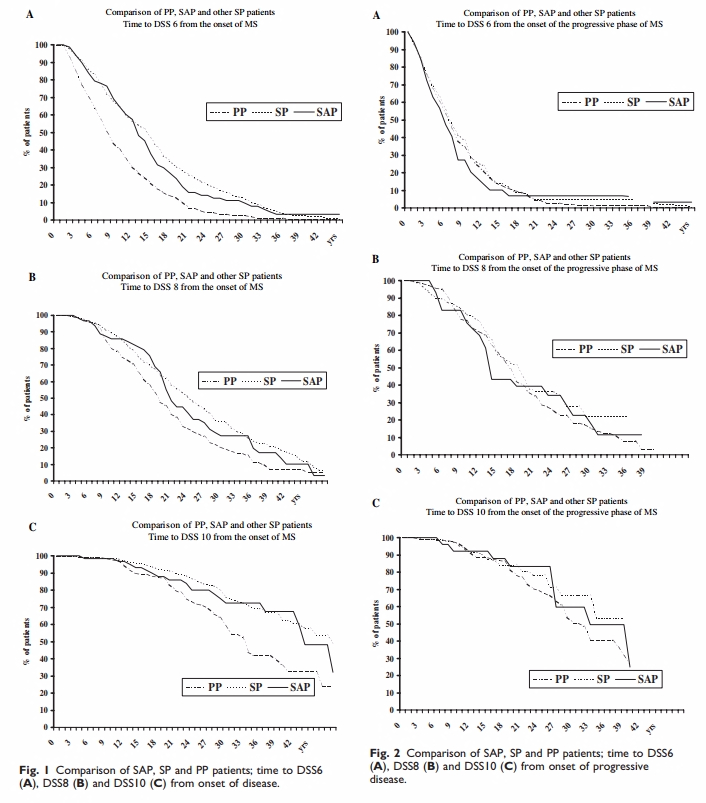
I often refer to the study below which showed that interferon-beta treatment, a moderate efficacy DMT, would probably work in PPMS provided the follow-up is long enough; in this case 7 years. In this study PwPPMS who had only been treated with IFNbeta for 2-years clearly did better at 7-years than those people treated on placebo over the same period of time. There was a lag in the impact of interferon-beta on the outcome.
Why a lag? One interpretation is that the impact of anti-inflammatory medications in progressive MS may take several years to play out. In other words progression in someone with PPMS over the next 2 years was primed by inflammation from years ago. Suppressing inflammation today will have no impact over the next 2-years as the damage priming progression over the next 2 years has already occurred. All anti-inflammatory therapies will have a lag in terms of showing a treatment response in progressive MS.
Does this make sense?
To illustrate this concept I drew the picture below, which has now been published in our length-dependent axonopathy paper. Importantly in this study, the actively-treated subjects (INF-beta) only did better than placebo-treated subjects in terms of upper limb function (9HPT), cognition and brain volume loss. There was no difference in terms of the EDSS and T25FW, which assess lower limb. The reason why there was no difference in lower limb function is almost certainly due to loss of reserve, i.e. too many nerve fibres supplying the limbs had been damaged already for an anti-inflammatory to make a difference. The other issue is that in this study the treatment period was too short. Please note this study is only one of many studies showing the same effect, a greater impact of anti-inflammatory therapies on upper limb, compared to lower limb, function and is one of the reasons we are running our #ThinkHand campaign and trying to get support for our CHARIOT-MS study.
In the ocrelizumab PPMS, ORATORIO, trial the treatment effect was almost double in the arms compared to the legs. This is why I have little doubt that ocrelizumab is effective in PPMS. If the trial was extended for longer the treatment effect on lower limb function will have gotten greater simply because of lag; survival or Kaplan-Meier curves diverge further with time.
I am convinced we are correct about ‘therapeutic lag’ and the MS community is beginning to take this it into account when designing progressive MS trials. This means being clever about our studies and getting the regulators to accept the 9HPT as a primary outcome measure. The MS community has made it clear that they value arm and hand function more than leg function, we now need the wider community to help get this message across. There is also an economic argument for taking DMTs into wheelchair users to protect upper limb function; once people lose their arm function they lose their independence and the costs, both medical and social, for looking after these become very high.
Just imagine what happens to your self-esteem and quality of life when you can’t transfer your self from your wheelchair to the toilet and need a carer to help you go the toilet? When we asked people with MS what hand and arm function they valued most many pwMS stated being able to go the toilet without help.
If you are a wealthy philanthropist reading this post? DrK (@KlausSchmierer) is looking for a large donation of ~£2M to support his application to the NIHR for the CHARIOT-MS study. He needs to bring the costs of the study for NIHR down to under £2.5M to have any chance of getting this trial funded and to help people with more advanced MS.
OBJECTIVES: To investigate, during the 5-year period without treatment after termination of a 2-year clinical trial of interferon beta-1b for the treatment of PPMS.
MAIN OUTCOME MEASURES: After 5 years without treatment, the EDSS and MSFC measures were scored for 63 and 59 MSers, respectively. Neuropsychological and magnetic resonance imaging assessments were performed for 59 and 50 MSers, respectively.
EDSS = Expanded Disability Status Scale
MSFC = MS Functional Composite ( a composite 3 tests the PASAT, 9-hole peg test and the timed 25-ft walk)
9-Hole Peg Test = test of upper limb function
Word List Generation Test = cognitive task
RESULTS: After 5 years without treatment, the interferon beta-1b group had better 9-Hole Peg Test (p=0.02) and Word List Generation Test (p<0.001) scores, and MRI measures in the normal-appearing white matter were significantly better. During the entire study period (from trial baseline to assessment at 5 years without treatment), the placebo group showed a greater decrease in brain volume (p=0.004). The in-trial increase of lesions correlated with the worsening of the EDSS score during the 5-year period without treatment (p =0.004).
CONCLUSIONS: Modest but beneficial effects of interferon beta-1b on clinical variables and brain atrophy development were observed 5 years after trial termination. Moreover, in-trial lesion activity correlated with EDSS progression after trial termination. Therefore, we provide evidence to consider immunomodulation as a sensible approach to treat primary progressive multiple sclerosis.
CoI: multiple