Barts-MS rose-tinted-odometer: ZERO-★’S (Black Tuesday – a tear for my beloved country #000000)
As you are aware by now I am a proponent of flipping the pyramid and using high-efficacy DMTs first-line including immune-reconstitution therapies (IRTs) such as alemtuzumab and AHSCT. I justify the latter two options based on the fact that given sufficient time the vast majority of pwMS will become disabled and the real cost of MS to people with MS cannot be underestimated; loss of employment, poor relationships, cognitive impairment, fatigue, depression, anxiety, etc. I think you get the gist; MS is a bad disease.
Alemtuzumab and HSCT are the two standout treatment options that offer pwMS the best chances of long-term remission and in some pwMS it may offer a cure. What impresses me about these two options is their impact on the end-organ, i.e. brain volume loss. After rebaselining at 12 months, pwMS treated with these two options lose brain volume on average at a rate that is within the normal range for age. The other DMTs don’t do this. The downside is that these two treatment options come with more risks. These two real-world studies below report 2 deaths out of 121 (2.5%) alemtuzumab-treated patients in Finland and 3 out of 120 HSCT-treated patients in London. Would you be willing to take these chances of dying to treat your MS with the potential for long term remission, possibly a cure and to protect your most precious end-organ the brain?
Background: Alemtuzumab is an effective disease-modifying therapy (DMT) for highly active multiple sclerosis (MS). However, safety concerns limit its use in clinical practice.
Objectives: To evaluate the safety of alemtuzumab in a nationwide cohort of Finnish MS patients.
Methods: In this retrospective case series study, we analyzed the data of all but two MS patients who had received alemtuzumab in Finland until 2019. Data were systematically collected from patient files.
Results: Altogether 121 patients were identified, most of whom had received previous DMTs (82.6%). Median follow-up time after treatment initiation was 30.3 months and exceeded 24 months in 78 patients. Infusion-associated reactions (IARs) were observed in 84.3%, 57.3%, and 57.1% of patients during alemtuzumab courses 1-3, respectively. Serious adverse events (SAEs) were observed in 32.2% of patients, serious IARs in 12.4% of patients, and SAEs other than IARs in 23.1% of patients. Autoimmune adverse events were observed in 30.6% of patients. One patient died of hemophagocytic lymphohistiocytosis, and one patient died of pneumonia. A previously unreported case of thrombotic thrombocytopenic purpura was documented.
Conclusions: SAEs were more frequent in the present cohort than in previous studies. Even though alemtuzumab is a highly effective therapy for MS, vigorous monitoring with a long enough follow-up time is advised.
Objective: to examine outcomes in people with multiple sclerosis (PwMS) treated with autologous hematopoietic stem cell transplantation (AHSCT) in a real-world setting.
Methods: retrospective cohort study on PwMS treated with AHSCT at two centers in London, UK, consecutively between 2012 and 2019 who had ≥ 6 months of follow-up or died at any time. Primary outcomes were survival free of MS relapses, MRI new lesions and worsening of expanded disability status scale (EDSS). Adverse events rates were also examined.
Results: the cohort includes 120 PwMS; 52% had progressive MS (primary or secondary) and 48% had relapsing-remitting MS (RRMS). At baseline, the median expanded disability status scale (EDSS) was 6.0; 90% of the evaluable cases showed MRI activity in the 12 months preceding AHSCT. Median follow-up after AHSCT was 21 months (range 6-85). MS relapse-free survival was 93% at 2 years and 87% at 4 years after AHSCT. No new MRI lesions were detected in 90% of subjects at 2 years and 85% at 4 years. EDSS progression-free survival (PFS) was 75% at 2 years and 65% at 4 years. EBV reactivation and monoclonal paraproteinemia were associated with worse PFS. There were 3 transplant-related deaths within 100 days (2.5%), all following fluid overload and cardiac or respiratory failure.
Conclusions: efficacy outcomes of AHSCT in this real-world cohort are similar to those reported in more stringently selected clinical trial populations, although the risks may be higher.
Classification of evidence: this study is rated Class IV because of the uncontrolled, open-label design.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.
Barts-MS rose-tinted-odometer: ★★★★★ (aquamarine on a very rainy Friday in London, #00FFBF)
I recently had a patient of mine who has been desperate to be treated with alemtuzumab actually ask if he can change his mind and rather be referred for AHSCT (autologous hematopoietic stem cell transplantation). Why? Because the chances of being put into long term remission, and hence potentially being cured of having MS, seems to be much higher with AHSCT. This particular patient has no concerns about the risks associated with alemtuzumab or AHSCT. The most important concern on his radar is his long term outcome. He wants a healthy brain when he gets older.
This is why this most recent paper on the long term outcome of Italian patients who received AHSCT adds to the mounting evidence base of the effectiveness of AHSCT. In patients with relapsing-remitting treated with AHSCT, MS 86% and 71% were free of disability worsening at 5 and 10 years, respectively. These figures for patients with progressive MS were 71% and 57% at 5 and 10 years, respectively.
The results are less impressive when using NEDA-3 status, i.e. no relapses, MRI activity or disability progression. For patients with RRMS, probabilities of achieving NEDA3 status were 62% at 5 years and 41% at 10 years, respectively. However, and importantly, in the subgroup of patients with RRMS who underwent AHSCT with the BEAM+ATG conditioning protocol, which is more aggressive, NEDA-3 status was achieved in 68% and 55% of subjects at 5 and 10 years, respectively.
In subjects with progressive MS, NEDA-3 status was only achieved 51% and 37% of subjects at 5 and 10 years, respectively.
On average, disability scores improved in relapsing-remitting subjects and got worse in subjects with progressive disease, which implies that AHSCT does not stop smouldering disease. However, almost all subjects had failed one or more DMTs prior to AHSCT. The latter is important. The average EDSS was ~6.0 and most patients had a disease duration of longer than 10 years. This makes me wonder how better the results would be if AHSCT was done earlier in the course of MS, i.e. before too much damage to the brain and spinal cord had accumulated. This is why we really need to test AHSCT as first-line therapy in MS. Could AHSCT done early stop/reverse or prevent the establishment of smouldering disease? In other words, does AHSCT cure people from having MS? This is why a trial of AHSCT in very early MS, i.e. as a first-line treatment, is a no-brainer to me.
Please note that three deaths occurred due to AHSCT, which was 1.4% of the entire study population.
The take home messages are:
AHSCT is the most effective DMT we have for treating MS.
RRMS responds better to AHSCT than progressive MS.
BEAM+ATG conditioning protocol is superior to cyclophosphamide-based protocols.
Mortality remains relatively high with AHSCT.
The results would be much better than this if patients had had AHSCT earlier in the course of their disease.
I was criticised yesterday for suggesting lifestyle changes to pwMS when I had no idea what it was like to have MS. It was implied that unless you have lived with MS, i.e. the lived experience, I shouldn’t be making any lifestyle recommendations to pwMS particularly around weight loss and diet. What I can say is that I have treated and followed thousands of people with MS and I know enough that if I had MS I would have no hesitation in wanting to be treated first-line with AHSCT or alemtuzumab and to manage all the lifestyle issues I referred to in my post ‘ASK NOT‘.
What underpins my decision to be treated with alemtuzumab and AHSCT first-line is the data missing from this paper on the end-organ; both of these treatments will on average normalise brain volume loss in treated subjects. In other words, these treatments are on top of the ladder when it comes to preventing end-organ damage. The downside of AHSCT is that the brain takes a significant neurotoxicity hit from the chemotherapy with accelerated brain volume loss in year one. In addition, there is also the high, but delayed secondary malignancy risk and high mortality risk associated with AHSCT that needs to be taken into account. Therefore, alemtuzumab probably wins out on safety as a potential first-line therapy. Please remember being treated with alemtuzumab does not exclude you from being treated with AHSCT at a later stage.
Objective: To determine whether autologous hematopoietic stem cell transplantation (aHSCT) is able to induce durable disease remission in people with multiple sclerosis (MS), we analyzed the long-term outcomes after transplant in a large cohort of MS patients.
Methods: To be included, a minimum data set (consisting of age, MS phenotype, EDSS at baseline, information on transplant technology and at least 1 follow-up visit after transplant) was required.
Results: 210 patients were included [relapsing-remitting (RR)MS=122(58%)]. Median baseline EDSS was 6(1-9), mean follow-up was 6.2(±5.0) years. Among RRMS patients, disability worsening-free survival (95%CI) was 85.5%(76.9-94.1%) at 5 years and 71.3%(57.8-84.8%) at 10 years. In patients with progressive MS, disability worsening-free survival was 71.0%(59.4-82.6%) and 57.2%(41.8-72.7%) at 5 and 10 years, respectively. In RRMS patients, EDSS significantly reduced after aHSCT [p=0.001; mean EDSS change per year -0.09 (95%CI=-0.15 to -0.04%)]. In RRMS patients, the use of the BEAM+ATG conditioning protocol was independently associated with a reduced risk of NEDA-3 failure [HR=0.27(0.14-0.50), p<0.001]. Three patients died within 100-days from aHSCT (1.4%); no deaths occurred in patients transplanted after 2007.
Conclusions: aHSCT prevents disability worsening in the majority of patients and induces durable improvement in disability in patients with RRMS. The BEAM+ATG conditioning protocol is associated with a more pronounced suppression of clinical relapses and MRI inflammatory activity.
Classification of evidence: This study provides Class IV evidence that for people with MS, aHSCT induces durable disease remission in most patients.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.
Barts-MS rose-tinted-odometer: ★ (milk chocolate; bitter-sweet and addictive)
I often refer to MS as being a pink-ribbon disease as close to 70% of pwMS are women.
The rising sex ratio from approximately 1:1 at the turn of the last century to almost 3:1 in most high MS incidence countries and to close to 5:1 in some areas of the world where the MS epidemic is still raging, justifies the pink-ribbon label. Explaining the rising female-to-male sex ratio really challenges those of us who think about MS and causation theory. If EBV is the cause of MS how does the EBV hypothesis explain the changing sex ratio? If you have any explanations or theories to explain the changing MS sex ratio I would be very very keen to hear them.
AHSCT or autologous haematopoietic stem cell transplantation has been getting quite a lot of air time recently. It is because it is such an effective treatment with the majority of people treated becoming NEDA, i.e. having no evident MS disease activity, and having the rate of their brain volume loss ‘normalised’ to be within the range of what you expect as a result of normal ageing. I am beginning to refer to this as NEO-EOD (no evident ongoing end-organ damage).
The problem with AHSCT is its safety profile and its associated adverse events (AEs). Despite the enthusiasm for AHSCT treatment from its very vocal supporters, the associated serious AEs are not trivial. The one AE that is the most troubling and often results in female patients saying no to a referral for AHSCT is the infertility risk. The chemotherapy used to mobilise haematopoietic stem cells and to ablate the immune system is toxic to the gonads. Men can easily bank sperm, but for women, the procedure of egg harvesting and egg banking is not trivial and it is expensive. In addition, many healthcare providers don’t cover the costs of banking; even in the UK, the latter is an NHS post-code lottery with some CCGs paying where others don’t.
Therefore, some pwMS simply take their chances with fertility. I am aware that the London haematologist that sees most of our patients quotes a figure of 40-45% for the rate of premature ovarian failure post-AHSCT. I think this figure is based on all non-cancer patients and is not necessarily specific to pwMS. Therefore it is reassuring to see the study from Italy below showing the rate to 30%, i.e. 70% of women with MS who are treated with AHSCT recover their menses. I suspect this is only half the story because the women who start to menstruate again may still be at risk of POF (premature ovarian failure) because the chemotherapy will have reduced their ovarian reserve, by culling a proportion of the ovaries oocytes or eggs. So this figure of 30% will increase with time and may end up being 45% or higher.
So it is not just about expanding access to AHSCT that is the issue but managing the AEs such as infertility that complicate the wide adoption of AHSCT for the treatment of MS. This is why I find patients tend to choose alemtuzumab over AHSCT when all of the pros and cons are presented side-by-side. So when you frame MS treatments with AHSCT as being the most effective treatment on the right people often move to the left and choose a treatment that may be less effective, but safer and unlikely to affect their fertility.
Please note I say alemtuzumab may be less effective, but I could easily say as effective, as AHSCT. Until we compare these treatments head-2-head we won’t know which is more effective. What I can say is that alemtuzumab and AHSCT are the most effective DMTs at rendering pwMS NEO-EOD.
Data on fertility after autologous hematopoietic stem cell transplantation (aHSCT) in women with multiple sclerosis (MS) are inconclusive. This study aims to report on post-aHSCT menstrual resumption in a multi-center MS-women cohort. Out of 43 women, 30 (70%) recovered menses after a mean time of 6.8 months. Older age (odds ratio (OR) = 0.5, p < 0.0001) and previous pulsed cyclophosphamide (OR = 0.44, p = 0.005) were independently associated with a reduced menstrual recovery probability. Conditioning regimens’ intensity resulted not associated with post-procedure amenorrhea. Our results highlight younger age as significantly associated with menses recovery; proper fertility counseling for MS women candidates to aHSCT both prior- and post-transplantation is therefore warranted.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
Barts-MS rose-tinted-odometer: zero-★’s – still seeing red
When the EMA doubted its wisdom and ran scared on alemtuzumab, after an Article 20 review of its benefits and risks, I was inundated with emails and queries.
“Gavin, didn’t you see this coming? Surely, alemtuzumab should never have been licensed as a 1st-line treatment for active MS? Clearly, the FDA got this right and the EMA made a mistake?”
What we are all forgetting in this debate is how bad MS can be as a disease and most of the early damage occurs occultly before people with the disease and their close ones realise the extent of the damage. What is lost in MS is lost forever. We have no magic treatment that can repair the damage and turn back the clock, which is why the Article 20 alemtuzumab review was so critical for the field. By the regulator’s taking away the ability of pwMS to assess and weigh up their own risks, and choose alemtuzumab first-line, has turned back the clock. In the UK alemtuzumab can only be used as a first-line agent in patients with rapidly evolving severe (RES) MS (two disabling attacks in a 12 month period), which is now a very small group of patients.
Early effective treatment in MS is about prevention; preventing the accrual of irreversible damage and giving pwMS the opportunity to age relatively normally. Now that alemtuzumab has become a 2nd- or 3rd-line option for pwMS many are seeking alternative treatment strategies and it has increased health tourism abroad for AHSCT. Is this what the EMA wanted?
As AHSCT is a procedure and not a drug, it doesn’t require EMA or MHRA approval. Therefore, we should be actively pushing for AHSCT to become a 1st-line treatment option. If I had MS, why would I want to watch and wait whilst I failed one or two DMTs before getting to the very high efficacy IRTs (immune reconstitution therapies) that have the biggest impact on preventing end-organ damage, reversing disability, inducing long-term remission and possibly offering a cure? Interestingly, both of these treatment options are considered to be the most cost-effective DMTs available.
When asked which DMT would I choose if I had MS, I have started saying AHSCT. When I admitted this a few years ago one of my patients, who I have been looking after for over a decade, sent me an email stating how upset she was that I had never offered her AHSCT. I clearly need to explain my position so as not to upset anyone else.
AHSCT is not on offer as a routine NHS therapy. At the moment AHSCT is only considered a 3rd-line treatment in the most active patients. Another problem is that it is not on offer across the country. There are only a handful of MS centres that are prepared to refer their patients for AHSCT. This means that access to AHSCT is not equitable and explains why an increasing number of patients travel abroad, at great personal cost, to receive this therapy.
The block in access to AHSCT seems to be at the level of the neurologist/MSologist. NHS England guidelines for bone marrow transplant (BMT) units allow them discretionary use of up to 15% of their AHSCT procedures to treat autoimmune conditions, which includes multiple sclerosis. As BMT units exist across the country access to these units would simply require a referral from a neurologist to the unit to request AHSCT as a treatment for MS. The latter, however, is unlikely to happen unless the local MSologist champions AHSCT as a procedure and gets their local haematology unit on board. It always takes a local champion to make things happen.
Another factor that has changed in the last 10 years is the strength of the evidence demonstrating how effective AHSCT really is as a treatment for MS. The MIST trial, the first large randomised controlled trial, and several meta-analyses of AHSCT confirm that AHSCT is a very effective therapy. At the same time, the risks associated with AHSCT have improved and the mortality in most BMT units is now below 1% for MS. This has now tipped the scales in favour of AHSCT becoming a mainstream treatment for MS.
There is however resistance from the MS community about AHSCT being offered as first-line therapy. Why? I suspect because the risk: benefit profile of AHSCT has yet to be compared in a head-2-head study against our most effective licensed treatment, alemtuzumab. This is why we are starting a head-2-head study, the STAR-MS trial, of alemtuzumab or ocrelizumab vs. AHSCT in the hope of generating evidence. With the EMA making alemtuzumab 2nd/3rd-line this trial will almost certainly recruit too few patients on alemtuzumab for a direct comparison of alemtuzumab vs. AHSCT. I predict the majority of patients in the comparator arm will be on ocrelizumab. This would not be asking the same question as ocrelizumab is used as maintenance therapy and may in fact do very well against AHSCT; the trial is using clinical NEDA (no relapses or disease progression) as the primary clinical outcome. Ocrelizumab is pretty good in the short term at achieving clinical NEDA. For me, end-organ damage or brain volume loss in years 2 and 3, after rebaselining at 12 months, would be a much more informative outcome. Do you agree?
We know already that AHSCT will be more cost-effective than alemtuzumab and ocrelizumab, but will it be more effective and most importantly will it be safer? I suspect it may not be as safe in the short-term, but what about over a 10-20 year horizon? The one long-term AHSCT risk that worries everyone is the delayed secondary malignancy risk; cyclophosphamide that is used in both the stem cell mobilisation and ablation phases of AHSCT is a DNA alkylating agent and hence a mutagen. This is why long term follow-up data from the European Bone Marrow Transplant Registry will be so important to provide this information. The other downside of AHSCT is ovarian toxicity and infertility, which in my experience are the most common reasons for my patients saying no.
Please remember that most of the proponents of AHSCT as a treatment for MS recognise that the major benefits from treatment will only be derived if AHSCT is used early in the course of the disease. This explains why most BMT units don’t offer AHSCT to pwMS with more advanced, or progressive, MS. However, this has not stopped private, fee-for-service, units offering AHSCT to all-comers. If you have the money and are willing to travel abroad you will be able to find a BMT unit that will treat you. I think this is wrong and will not happen in the NHS if and when AHSCT becomes widely available. We have to be honest with our patients about the risks and the benefits of AHSCT and why we will limit AHSCT to those who will benefit the most. In fact, there is evidence that more advanced patients may actually be made worse by AHSCT; the chemotherapy used to ablate the immune system is neurotoxic and may speed up neuronal loss. In addition, serious life-threatening infections are more common when you have AHSCT, particularly in patients with more advanced MS, and infections are well known to worsen MS disability in more advanced disease.
Please be aware that AHSCT is not for the faint-hearted. It is a risky therapy with serious adverse events and quite a high mortality. Even a mortality rate of 0.3–0.5% is high when compared to licensed DMTs. Should this stop us from offering AHSCT first-line? I think not. If we have been prepared to offer alemtuzumab, with its risk profile as a first-line treatment, why not AHSCT? Most pwMS would agree that the decision regarding what is an acceptable risk to take should be taken by the patient and their families, and not the neurologist or other HCP. There is data showing that neurologists are much more risk-averse than pwMS. Neurologists need to acknowledge this bias, which is likely to be an unconscious bias, and let their patients make the decision.
What I am really trying to do by stating that if I had MS I would choose AHSCT as my treatment is to reframe the DMT debate, particularly in relation to access to highly effective DMTs. By focusing on AHSCT as a first-line treatment it should at least make you consider what your treatment objectives are in MS.
Framing is another cognitive bias that was identified by Daniel Kahneman, the Nobel laureate, and his partner Amos Tversky. By moving the frame upwards, or to the right, i.e to include AHSCT as a 1st-line therapy, it makes it more likely for pwMS and their neurologists to choose more effective, but arguably safer, treatments 1st-line.
We now know that people who start on a low to moderate efficacy DMT do worse on average than those who start on a high or very high efficacy therapies do better. Despite this, the majority of pwMS are not told this and are started on a low efficacy or platform DMTs without ever being given the option of a high efficacy DMT. Why? It is not due to lack of access to treatments as we now have several NICE and NHS England approved high efficacy DMTs available as first-line treatments.
So yes, if I had active MS I would want to have the full spectrum of high-efficacy DMTs available to choose from including AHSCT. I would want to know about their relative efficacy and what the aim of the treatments are. I would certainly want to have a discussion about the possibility of a potential cure.
By reframing the spectrum of efficacy by including AHSCT within the frame we may nudge pwMS and their neurologists to move up the treatment ladder and choose a high efficacy DMT sooner when they have more brain to protect.
Unfortunately, AHSCT as a first-line option is not going to happen any time soon, unless the MS community starts debating the issue in earnest. I am not alone, or out on a limb with my position; I have a short, but growing list, of MSologists who have told me that if they had MS they would want AHSCT first-line. If your MSologist would like his/her MS treated with AHSCT, why wouldn’t you?
PS: this blog post is adapted from a Medium post ‘Framing the DMT debate’ published on the 15th April 2019.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
Shortly after leaving Queen Square to take up my current position at Barts and The London Juliet Solomon, a good friend, and one of the research managers who had an office opposite me on the 6th floor of the Institute of Neurology sent me a signed copy of the ‘The Book of Regrets’ she had compiled as a present. She has asked celebrities to write essays on something they had regretted in their lives. The book has become a bestseller with all the proceeds of the sales going to support the National Hospital for Neurology and Neurosurgery. This is the kind of thing Juliet does; she has a very big heart. A mensch!
At the time I thought about what I would write if I was asked to contribute a chapter to the next edition of the book. I am still not sure, but from a professional perspective, my biggest regret is not being more proactive in derisking alemtuzumab as a treatment for MS. It has become clear to me that a small proportion of people with MS (pwMS) who are treated with alemtuzumab and HSCT early in the course of their disease are cured of MS when you use a contemporary definition of an MS cure.
If the infusion reactions, infections and secondary autoimmunity problems went away who would choose anything but alemtuzumab to treat their MS?
Infusion reactions: Can we reduce the infusion reactions of alemtuzumab? Yes, we can. Pre-treating with steroids starting the night before and moving from the intravenous to the subcutaneous route would make infusion reactions minor. So why hasn’t this been done? Money! MS centres/units make lucre out of infusing patients. I have used the subcutaneous route to avoid a second about of steroid-induced psychosis, to avoid steroid-induced metabolic mayhem in a patient with MS and type 1 diabetes and in a patient who developed avascular necrosis of one hip after his first course of alemtuzumab. It was remarkable; there were no major alemtuzumab infusion reactions despite these three patients being steroid-free. The pharmacodynamic data, i.e. the cell depletion data for the IV and SC routes are identical. The main reasons for us not switching all our patients to subcutaneous alemtuzumab was money, resource and inertia. In the recent past, we used to make money for the unit by giving infusions. Fortunately, with NHS block contracts, this perverse incentive has disappeared. Sanofi-Genzyme also provides contract nurses who come in to give the infusions and monitor the patients. If we converted our entire alemtuzumab administration programme to a subcutaneous route the workload would fall on our overworked nurses. Our nursing lead in our daycare unit reminded me of this. REGRET 1 we didn’t covert to sc alemtuzumab.
Secondary autoimmunity: What about preventing or reducing the incidence of secondary autoimmunity?
The immune system has many mechanisms in place to prevent autoimmunity. When you learn how the immune system works it is really quite surprising that autoimmunity is so uncommon. What the immunologists tell us is that there must be a series of underlying biological processes that are causing secondary autoimmunity and if we can work out what these are we can intervene and prevent this complication. This is what Joanne Jones and Alasdair Coles tried to do in Cambridge. Their hypothesis was that because the immune system reboots itself from peripheral memory cells it is more likely to result in an aberrant autoimmune response. They tried rebooting the immune system using more naïve cells from the thymus using the hormone palifermin, which stimulates the thymus to produce more naïve T-cells. Sadly it didn’t work, but at least they tried and they should be congratulated for doing this study.
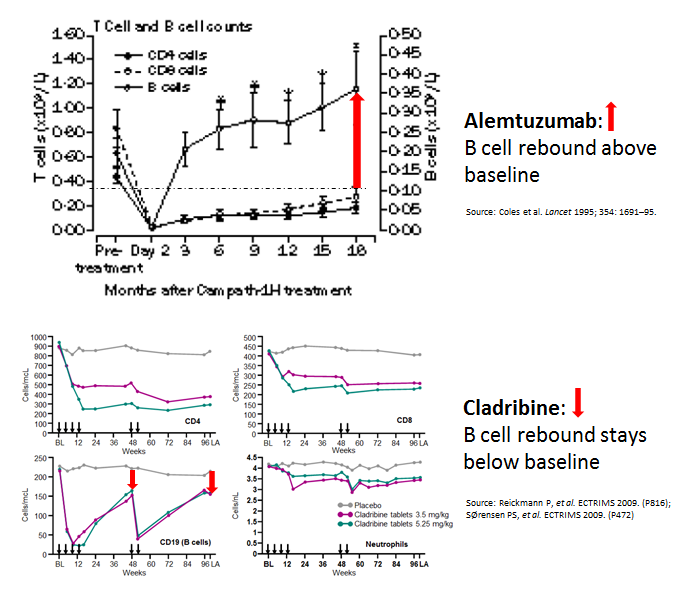
Interestingly, when you compare cladribine, another IRT, with alemtuzumab you can’t help but notice that the B-cell reconstitution profiles are very different. With alemtuzumab, they come back very quickly and overshoot their baseline values. We, and others, have hypothesised that if you change the profile of the B cell reconstitution with a small dose of the B cell depleting antibody rituximab you may be able to prevent this secondary autoimmunity. We are really talking about a very small dose of rituximab, i.e. 10-20mg, just enough to delay B cell reconstitution by 4-6 months. I proposed this concept to Genzyme 8 or 9 years ago, but without data to support the hypothesis they were not keen to support an exploratory study. Why didn’t I push to get this funded from another source? If we had done this study back then we would have had the results by now. Can you imagine how impactful this could be for pwMS if we could prevent secondary autoimmunity post-alemtuzumab? REGRET 2 no doing alemtuzumab-rituximab trial and not setting up an adaptive trial platform for testing multiple strategies to prevent secondary autoimmunity post-alemtuzumab.
Infections: One success story has been the derisking of alemtuzumab-associated infections with prophylactic antibiotics and antivirals, and the proactive approach to baseline infectious disease screening and vaccination. SUCCESS 1 reducing alemtuzumab-associated infections.
Anti-drug antibodies: Another success story has been exposing alemtuzumab’s problems with anti-drug antibodies (ADAs) and the development of an assay to screen for these antibodies. Why use a therapy, at great expense, that is not going to work because of neutralizing anti-drug antibodies. SUCCESS 2, anti-drug antibody screening.
A big problem that emerged was how alemtuzumab was licensed and used in the USA. The FDA has essentially licensed alemtuzumab with hand-cuffs, therefore, alemtuzumab was and is used as the DMT of last resort in the US. This led to it being used in an older more advanced cohort of pwMS who had comorbidities. In this group of patients, a new adverse event profile emerged, particularly vascular complications. This led to a safety review and the license of alemtuzumab’s use was changed and it is now only used infrequently, second or third -line and often in people with more advanced MS. I was personally involved with the original EMA submission; it was a real uphill battle to get alemtuzumab licensed as first-line therapy. Allowing the EMA to change how we use alemtuzumab, i.e. making pwMS have to wait to become eligible for the therapy is a travesty. We, Genzyme and MS community, should have made a more robust argument to the CHMP not to change alemtuzumab’s label. REGRET 3 not allowing alemtuzumab to be used first-line in active MS; it can only be used as a first-line agent in patients with rapidly evolving severe (RES) MS (two disabling attacks in a 12 month period). The problem is that very few patients have RES MS as they tend to be treated now before they have their second disabling relapse.
Finally, my colleagues. Apart from a small group of MSologists, and we know who we are, most MSologists don’t prescribe alemtuzumab. They find the therapy too difficult and risky to use. I have tried to educate and get more of my colleagues to at least offer alemtuzumab as an alternative to HSCT, but to no avail. In the UK, we were all geared up to do a head-2-head study of alemtuzumab vs. AHSCT. However, once ocrelizumab was licensed the MS community said they would not be able to recruit for this trial so it has now been converted into alemtuzumab or ocrelizumab vs. AHSCT trial. In reality, this study is going to be a head-2-head of ocrelizumab vs. AHSCT study. Not getting the wider MS community to understand how effective alemtuzumab is REGRET 4. Instead of success, we have a generation of refuseniks.
The question we need to ask ourselves is do we really want to throw the baby out with the bathwater? We have two, and possibly three, treatment strategies that may cure a minority of pwMS of having MS. Yes, CURE. However, alemtuzumab and HSCT are on the fringe of MS treatments. Why?
I suppose you are asking about the third option. It may be cladribine. The results of the ORACLE trial of cladribine in patients with clinically isolated syndromes (CIS) are quite remarkable. We are trying to recall the patients from the ORACLE study a decade or more later to see how many are still in remission and haven’t converted to MS. The problem we have is that cladribine is not even a treatment option for CIS despite this stunning data, hence we may be denying a large number of people with CIS, a relatively safe immune reconstitution therapy or IRT, that may prevent many of them from developing MS. The downside of this is the depressing fact that many MSologists still don’t treat CIS (see my blog post on watchful waiting).
Alemtuzumab is an anti-CD52 monoclonal antibody with remarkable efficacy in relapsing multiple sclerosis (MS). In clinical trials and off-label use in MS, alemtuzumab has been administered intravenously (IV). Alemtuzumab is approved for chronic lymphoid leukemia as IV. Oncology guidelines recommend alemtuzumab subcutaneous (SC) over IV. There is no report of alemtuzumab SC in MS. We report two patients with highly active relapsing MS who were treated with SC alemtuzumab, had significant improvement and tolerated SC alemtuzumab well without the typical infusion-associated adverse events. SC alemtuzumab in MS warrants further studies as this may enhance patient convenience and minimize infusion-associated adverse events.
Background: Patients who develop relapsing-remitting multiple sclerosis (MS) present with a first clinical demyelinating event. In this double-blind, multicentre, randomised, phase 3 study we investigated the effect of oral cladribine on conversion to clinically definite MS in patients with a first clinical demyelinating event, when given at the same doses shown to be effective in relapsing-remitting MS.
Methods: Between Oct 21, 2008, and Oct 11, 2010, we recruited patients aged 18-55 years, inclusive, from 160 hospitals, private clinics, or treatment centres in 34 countries. Eligible patients had a first clinical demyelinating event within 75 days before screening, at least two clinically silent lesions of at least 3 mm on a T2-weighted brain MRI scan, and an Expanded Disability Status Scale score of 5.0 or lower. Patients with a first clinical demyelinating event ≤75 days before screening were randomly assigned (1:1:1) to receive cladribine tablets at cumulative doses of 5.25 mg/kg or 3.5 mg/kg or placebo. Randomisation was done with a central web-based randomisation system and was stratified by geographic region. Masking was maintained using a two-physician model. The primary endpoint of this 96-week study was time to conversion to clinically definite MS according to the Poser criteria. This study is registered with ClinicalTrials.gov, number NCT00725985.
Findings: Of 903 participants assessed for eligibility, 616 patients received cladribine 5.25 mg/kg (n=204), cladribine 3.5 mg/kg (n=206), or placebo (n=206). At trial termination on Oct 25, 2011, cladribine was associated with a risk reduction versus placebo for time to conversion to clinically definite MS (hazard ratio [HR] for 5.25 mg/kg=0.38, 95% CI 0.25-0.58, p<0.0001; HR for 3.5 mg/kg=0.33, 0.21-0.51, p<0.0001). Adverse events were reported in 165 (81%) patients in the cladribine 5.25 mg/kg group, 168 (82%) patients in the cladribine 3.5 mg/kg group, and 162 (79%) patients in the placebo group. We noted no increase in risk of adverse events with active treatment versus placebo apart from lymphopenia, which was a severe event in 10 (5%) patients in the 5.25 mg/kg group and four (2%) patients in the 3.5 mg/kg group.
Interpretation: Both doses of cladribine significantly delayed MS diagnosis compared with placebo. The safety profile of cladribine was similar to that noted in a trial in patients with relapsing-remitting MS. Further research could clarify the potential effects of oral cladribine treatment in the early stages of MS.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
There is little doubt in my mind that HSCT is the most effective DMT we have for treating MS. The latter is based on NEDA (no evident disease activity) rates post-HSCT and brain volume loss data after year one. HSCT appears to put the majority of treated patients into long-term remission and normalises end-organ damage as measured by brain volume loss. In addition, a not insignificant proportion of HSCT-treated patients may be cured depending on how you want to define an MS cure. Despite these data most MSologists however, consider HSCT too risky to refer patients for treatment and hence prefer to go with the more acceptable risk profile of licensed DMTs. This is why HSCT hasn’t taken off as a mainstream treatment for MS and remains a niche treatment.
What is not known is that HSCT may yet prove to be one of the most cost-effective DMTs we have. Although quite expensive, with most of the costs front-loaded, HSCT does lead to significant cost savings in the long-term (see study below). I wonder if healthcare systems will clock this and take the bold step of underwriting more HSCT treatments for MS with the promise of long term cost savings? The problem we have in medicine is that healthcare budgets typically run on an annual cycle and so costs savings unless made the same year often don’t influence treatment decisions.
“Why should I spend more money today to only save money in the 5 years time? My responsibility is to this year’s or maybe next year’s budget not the budget in 5 years time.”
The counter-argument to this is should be if I don’t save my brain volume this year or next year, by the time I get to year 5 in my disease course it will be too late. At the moment MS brain and spinal cord damage are irreversible. Yes, time really is brain.
What do you do as a person with MS who has decided to be treated with HSCT, but your neurologist says no? Do you find a neurologist who will say yes? Do you travel abroad and take the private route? Or do you accept your neurologist’s advice and go for the safer, but ultimately more expensive, licensed but less effective DMT?
The good news is that we in the UK will soon be starting the StartMS trial, which will compare autologous stem cell transplantation (AHSCT) versus alemtuzumab or ocrelizumab in relapsing-remitting MS. This means at least some of you will be offered the opportunity to be randomised to AHSCT or ocrelizumab/alemtuzumab. A major outcome of this study will be a cost-comparison to see how much money it will save the NHS. Exciting or not? Some people are arguing that we don’t need this study as the information is already available. Not sure I agree. Sometimes doing your own research and generating your own data is what is required to change behaviour, i.e. the wide adoption of HSCT as a treatment for MS.
Objectives: To provide real-world data on the impact of autologous hematopoietic stem cell transplantation (AHSCT) on treatment costs of patients with multiple sclerosis (MS) in Poland.
Methods: Medical data of 105 patients who underwent AHSCT in the years 2011 to 2016 were obtained from the National Health Fund (NHF) database. Treatment costs were calculated from the public payer’s perspective per patient-year for the total available period as well as 12 months before and after AHSCT. The statistical analysis was performed using MATLAB 2016b.
Results: Mean treatment-related costs covered by the NHF per patient-year before and after the transplantation were €4314.9 and €1188.8 , respectively. The average cost of disease-modifying drugs per patient was reduced from €2497.9/year before to €65.3/year after AHSCT.
Conclusions: Although the initial cost of AHSCT is high, the costs involving AHSCT and post-AHSCT treatment could, according to our analysis, pay off in 3.9 years, when compared to the costs of disease-modifying drug therapy in aggressive MS. The study provides evidence that the AHSCT can lead to significant savings in treatment costs of aggressive MS from the public payer’s perspective.
Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the position of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
Good news for people with MS living in the US. The National Multiple Sclerosis Society is acknowledging that autologous hematopoietic stem cell transplant (AHSCT) is an effective treatment for MS as is recommending AHSCT a useful treatment option for pwMS who have substantial breakthrough disease activity despite treatment with high-efficacy DMTs or have contraindications to high-efficacy disease-modifying therapies. The acknowledge that pwMS younger than 50 years with shorter durations of disease (<10 years) have the most to gain from AHSCT.
The big question is will insurers and national funders pay for HSCT in the US based on this recommendation or will they still need FDA approval?
The good news for pwMS living in the UK is that the NHS already covers the cost of HSCT and MS is on the list of approved autoimmune diseases for treatment with HSCT. The problem in the UK is not necessarily the access to the treatment, but to get risk-averse neurologists to refer pwMS for the procedure or am I wrong?
Importance: Autologous hematopoietic stem cell transplant (AHSCT) for multiple sclerosis has gained increasing interest in recent years. Despite the availability of many US Food and Drug Administration–approved disease-modifying therapies, some patients do not respond adequately and others may have very early aggressive disease that prompts consideration of alternative, highly effective, long-lasting therapy. The National Medical Advisory Committee of the National Multiple Sclerosis Society has reviewed recent literature on AHSCT for the purpose of making recommendations about its use based on current knowledge, as well as pointing out areas of controversy and issues requiring further research.
Observations: Studies on AHSCT have repeatedly demonstrated high efficacy and a durable outcome in people with relapsing multiple sclerosis. Recent studies have shown considerable improvement in the safety of the procedure, with much lower mortality rates than were reported earlier. Consensus is emerging about the characteristics of the best candidates for the procedure. Questions remain about the ideal protocol, particularly about the best conditioning regimen to be used to kill immune cells. Larger randomized clinical trials are needed to address the question of whether AHSCT has advantages over the most efficacious disease-modifying agents currently available. One such trial (Best Available Therapy Versus Autologous Hematopoietic Stem Cell Transplant for Multiple Sclerosis [BEAT-MS) is currently in progress.
Conclusions and Relevance: The National Multiple Sclerosis Society believes that AHSCT may be a useful treatment option for people with relapsing multiple sclerosis who demonstrate substantial breakthrough disease activity (ie, new inflammatory central nervous system lesions and/or clinical relapses) despite treatment with high-efficacy disease-modifying therapy or have contraindications to high-efficacy disease-modifying therapies. The best candidates are likely people younger than 50 years with shorter durations of disease (<10 years). The procedure should only be performed at centers with substantial experience and expertise. Ideally, recipients of the procedure should be entered into a single database, and further research is needed to establish ideal cell mobilization and immune-conditioning regimens.