“In response to several question on steroids and AVN (avascular necrosis of the hip) in MSers. Most neurology consultations are simply too short to discuss all the relevant issues, in particular preventive strategies for example bone health. We neurologists, tend to focus on the here and now. If you don’t agree with this then we need to change the way we practice. Do you want change?”
“We simply don’t have enough data to be able to say how common AVN is in MSers and at what dose of steroids, or number of courses of steroids, does the risk increase. The following is a small case series of 5 cases. I recall a case of Professor W. Ian McDonald’s, who I looked after, who developed bilateral AVN of the hips after only one course of high-dose methylprednisolone for a severe spinal cord relapse. He illustrates to me that AVN can occur after just one course. In addition to steroids other risk factors that are not relevant to MS include radiation therapy, chemotherapy, and organ transplantation (particularly kidney transplantation).”
“In the early stages of AVN, MSers may not have any symptoms. As the disease progresses, however, most experience joint pain. At first, the pain occurs only when putting weight on the affected joint. Later, it occurs even at rest. Pain usually develops gradually, and may be mild or severe. If AVN progresses and the bone and surrounding joint surface collapse, pain may develop or increase dramatically. Pain may be severe enough to limit range of motion in the affected joint. The period between the first symptoms and loss of joint function is different for each person, but it typically ranges from months to years.”
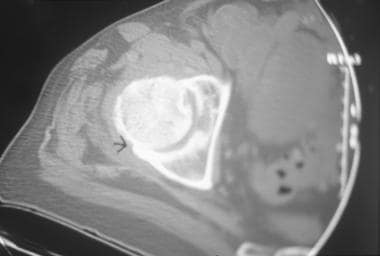
“AVN is usually diagnosed on history and examination followed by imaging. This is why well localised hip pain should be taken very seriously. The latter may include a plain hip x-ray, but a plain x-ray is typically normal early on. MRI or a CT is generally diagnostic and bone scan helps in that it identify other joints that are involved that are asymptomatic.”
“I suggest reading the NIH health information sheet for more information on AVN. The treatment of AVN is really symptomatic, but if the AVN is unilateral a core decompression of the opposite hip may prevent it becoming bilateral. However, not all orthopaedic surgeons agree with prophylactic decompression. It seems as if the evidence base regarding the latter is not black-and-white, but shades of gray; not too dissimilar to the field of MS.”
 |
| CT-scan: AVN of hip joint |
{kind=link}
Sahraian et al. Avascular necrosis of the femoral head in multiple sclerosis: report of five patients. Neurol Sci. 2012 Dec;33(6):1443-6.
Osteonecrosis of the femoral head is a severe complication of corticosteroids, which may lead to more disability in multiple sclerosis (MS) patients because of delayed diagnosis. The exact dose and risk period of steroids which cause the necrosis are not clearly known. The aim of the study was to enhance the attention of clinicians to leg pain in MS patients with regard to steroid therapies. We report five MS patients with femoral head necrosis who had relapsing remitting MS and received different doses of methylprednisolone. Our young cases consist of three females and two males. The duration of disease varied between 1 and 3 years. The least interval between the last pulse of prednisolone and diagnosis of avascular necrosis was 6 months. Two of them received one pulse of 5 g of methyl prednisolone. All five patients had delayed diagnosis because the signs and symptoms were attributed to MS, which indicate the necessity of further focusing attention to early evaluations.
At the very least, we should be told of the risks of taking steroids. I hadn't even heard of AVN. In my ignorance, I thought the main danger of steroids was weight gain after years of continuous usage.
Yes, I want change. What can we do to make neurologists tell us everything?
Thanks for answering – fingers crossed that 5 days for of methylpred given with alemtuzumab isn't a problem. I'll be a bit antsy if my early effective treatment leaves me immobile!If it was common surely it would have been flagged in the trials?
Prof G, you've asked the question do we want change? I refused steroids under the care of Prof Macdonald, but later needed them for a relapse. I had a fair idea of anything that required me to carry around a card showing my medication wasn't a great thing. I feel we will carry on regardless. The actual issue is, that we don't know why MS patients develop Osteoporosis and it is assumed we live a sedentary lifestyle. The litigation culture we find ourselves in is doing us no favours. Is anyone willing to do the research? I guess not.
Osteoporosis?
All very interesting or should I say potentially alarming for people who have taken steroids. But how about information on how to mitigate steroid induced osteoporosis? This is a link to some information http://patient.info/health/preventing-steroid-induced-osteoporosisI'm slightly relieved that I'm very active and run 3 times a week and walk every day for miles, and I've never broken a bone or even twisted an ankle. My Vit D is in the optimum range (measured every 6 months) but as I'm getting older and have taken around four treatments with steroids over the years, I'm going to request a bone scan (my GP will love me!!)
Did all I could still got Osteoporosis. No family history.
My wife was diagnosed with Ms 9 years ago and has gone from remitting relapsing ms to secondary progressive ms and has had no feeling from the waist down until about 18 months ago when she has had pain in her hips and leg joints. Recently she has had a pressure wound which has turned Necrotic 3cm by 3.5cm depth unknown she has had steroids in the past I was wondering if these steroids could be the cause if it was undiagnosed? should we ask for a bone scan?
My wife was diagnosed with Ms 9 years ago and has gone from remitting relapsing ms to secondary progressive ms and has had no feeling from the waist down until about 18 months ago when she has had pain in her hips and leg joints. Recently she has had a pressure wound which has turned Necrotic 3cm by 3.5cm depth unknown she has had steroids in the past I was wondering if these steroids could be the cause if it was undiagnosed? should we ask for a bone scan?
I plan to do a future series of posts on Bone Health; it will refer to osteopaenia, fractures and preventing avascular necrosis of the hip and other bones.
Avascular necrosis is diseases that damage the bone density by affecting the blood supply of the joint.it is also knows as osteonecrosis