Barts-MS rose-tinted-odometer: ★★ (amber; a sleep deprived colour somewhere between yellow and orange)

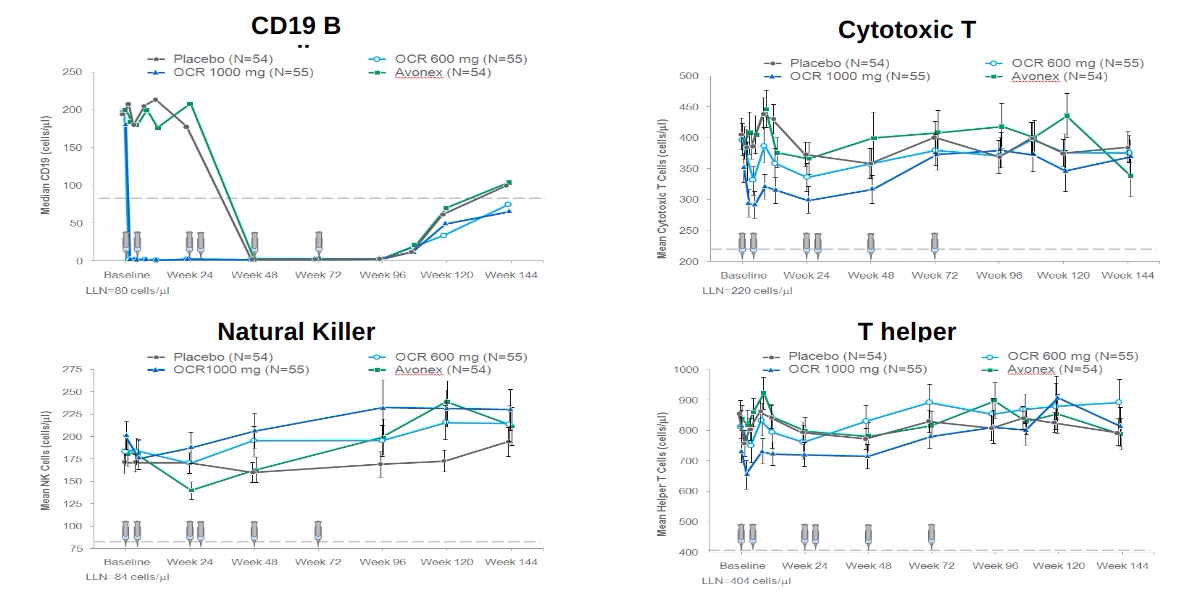
It has become clear that the anti-CD20 therapies are more than just anti-B-cell therapies. Minority populations of both CD4+ and CD8+ T-cells and NK-cells express CD20 and are depleted after both rituximab and ocrelizumab treatment.
It looks as if ocrelizumab may be more effective in deleting this population of cells and may explain why herpes zoster or shingles is more common after ocrelizumab, compared to rituximab, than what you would expect based on its putative B-cell only targeting effect. The mild depletion of this population of cells may also explain why pwMS on ocrelizumab are at higher risk of getting COVID-19 and severe COVID-19.

The study below shows that this population of cells express a so-called CTL or cytotoxic phenotype that fits in with the zoster and COVID-19 data. This also raises concerns that just maybe peripheral tumour immune surveillance is also compromised on anti-CD20 therapies. The tumour signal however is likely to be small as a large secondary cancer signal would likely have emerged already on the anti-CD20s.
More topical is the role these CD20-expressing T-cells play in vaccine responses. If they are important in vaccine immunity then patients with MS on anti-CD20 therapies who lack this population of T-cells may not develop adequate T-cell immunity in response to vaccination. We won’t have long to wait for the latter data as many immunology laboratories are busy trying to get their T-cell vaccine data out as soon as possible.
So yes there is much more to the immunology of anti-CD20 therapy than simple B-cell depletion. Could the T-cell compartment targeted by anti-Cd20 therapies be as important or more important than the B-cell compartment? There is so much more to learn about how MS DMTs really work, in particular the anti-CD20 therapies.
Boldrini et al. Cytotoxic profile of CD3+CD20+ T cells in progressive multiple sclerosis. Mult Scler Relat Disord. 2021 May 7;52:103013.
Recently, it was shown that highly effective anti-CD20 therapies used for MS patients not only deplete CD20+ B cells, but also a small subset of T cells expressing CD20 surface marker (CD3+CD20+ T cells). Here we demonstrated that, in progressive MS patients, CD3+CD20+ T cells share the ability to express cytotoxic factors such as perforin and serine-protease granzyme-B (GzmB), classically associated with CD8+ T cells functionality. Beyond it, cluster analyses show that a set of activation markers and transcriptional factors related with CD8 effector program are also expressed in CD3+CD20+ T cells. Further characterization of surface and functional markers from CD3+CD20+ T subsets may be helpful for development of new therapeutic strategies mainly for progressive MS patients, as well as for assessing pathophysiological effects of highly effective anti-CD20 therapies.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
In how many years should we expect to see the “start” of a phase 3 antiretroviral ( for ebv ) in ms ?
10-20 years
But you mentionned that a cure is « less » than 5-7 years away ? Also you mentionned in the smouldering ms video on YouTube that you would not be surprised if in 4-5 years time someone comes up with a strikingly positive trial of an antiviral drug ( which i thought you meant a phase 2 ) ? Also there is the tenofovir alafenamide trial happening right now ? So why 10-20 years?
The current trials are too small to be definitive. Running a pharma sponsored phase 2 (dose-finding), followed by a proper phase 3 programme takes 8-10 years. And then there is licensing and market access etc. Nothing happens quickly in relation to drug discovery. This is made worse by the potentially disruptive technology.
Okay I see and so why do you feel a cure could be here in less than 5-7 years time what did you mean by that ?
Prof G. – if an ELISPOT Assey confirms that you had a „significant“ reaction against Sars Covid Antigen (IfNg and IL2) then one has enough t-cells left after some rounds of OCR? or ist that assey not specific enough?
thank you!
It is specific enough and shows that the person has some T-cell immunity to the virus.
How long should we still wait to see the T-cell vaccine data in people on Ocrelizumab? I remember that back in March, they were expected to be released in April, then in May, now June is coming… Is there any publication or so? Thanks
Not sure. To the best of my knowledge, the labs are still doing the work. Likely to be presented at ECTRIMS later this year or possibly the EAN in June.
I have unfortunately seen worsening of symptoms after Cladribine treament but there is no evidence on MRI; is there any DMT I would be allowed to take to halt further deterioration? Ocrelizumab? Would you advise against the use of Ocrelizumab in an MS patient with more disabling MS and over 50 years of age because of accumulative risk of infections?
Re: “I have unfortunately seen worsening of symptoms after Cladribine…”
This is what we refer to as PIRA (progression independent of relapse activity) or more appropriately smouldering MS. This is the holy grail of MS. At the moment we have no known therapies that have been shown to work on this phase of the disease, which is why we are doing things such as the SIZOMUS trial.
Prof G,
“This is what we refer to as PIRA (progression independent of relapse activity) or more appropriately smouldering MS. This is the holy grail of MS. At the moment we have no known therapies that have been shown to work on this phase of the disease”.
If cladribine is not having an impact on PIRA (in the case above), why is it being tested on people with advanced MS whose worsening must be due to PIRA?
ChariotMS ‘Cladribine to halt deterioration in people with advanced MS’.
The emphasis here is on “no known” therapies. It is only through testing that we can find out.
Also worth noting that PIRA likely covers various processes, not only “smouldering” MS. There are evidently people with a progressive phenotype (no clinical relapses), yet plenty of outright inflammatory lesion activity. This is where we already have evidence in favour of cladribine; for example: https://pubmed.ncbi.nlm.nih.gov/29860198/.
Whether it also works on smouldering lesions? – We’ll find out through ChariotMS, where smouldering lesions are included as an exploratory outcome!
Re: “halt deterioration”
This is the ambition but is likely to slow deterioration. However, halting vs. slowing depends on the underlying reserve and if some subjects have a lot of reserve capacity in the neuronal pathways innervating the upper limbs it may halt worsening. You have to remember this is only the second trial to use the 9HPT as the primary outcome measure to assess the efficacy of a DMT.
“If cladribine is not having an impact on PIRA (in the case above), why is it being tested on people with advanced MS whose worsening must be due to PIRA?”
No-one will admit it but clearly it’s
Because they don’t have anything better to try.
Seen many post on FB…they worsen on Cladribine. Clear that it’s not enough to have a pill that
that depletes t and b cells to cure ms. Hsct seems better
shot to halt advanced ms than cladribine..unfortunate
someone posted their neuro told him to try Cladribine
before hsct and he had big edss progression..which
only hurt his hsct chances.
“Cladribine was approved by the FDA in 1993 for HCL hairy cell leukemia as an orphan drug,[19] and was approved in Europe later that year.”
Maybe there was a reason
it didn’t come out for ms back in 1990’s.
“Cladribine is an effective treatment for relapsing remitting MS, with a reduction in the annual rate of relapses of 54.5%.[12] These effects may be sustained up to 4 years after initial treatment, even if no further doses are given.[37]
https://en.wikipedia.org/wiki/Cladribine
I think that all DMT will find it hard to halt worsening in advanced MS because there are elements that will not resppond to such DMT, but I think the aim is to have impact on systems with reserve. We know that we need to protect and repair, but adding extra arms could not be done budget wise.
Anon – If your source is Wikipedia, your statements have zero credibility on a MS “research” blog.
HSCT is not a cure, it works for some and it does not work for others….just like all the other approved DMTs. Depends on the individual and their current disease course/severity. However, HSCT has a much higher (confirmed) death rate, unlike the other “approved” DMTs.
Please keep your negative comments to yourself and go troll some other blog.
Some of us actually have hope that one of these DMTs or procedures will slow down our progression, even if just a little. So we do not need your negativity, conspiracy theories, or trashing of highly effective drugs.
Come at me with real facts, not some BS you read on FB. If I posted on FB that the Earth was flat or the pandemic was fake would you believe me, or the scientist!!!!
Instead of reading Wikipedia and FB….maybe try educating yourself:
Potential mechanisms of action related to the efficacy and safety of cladribine.Baker D, Pryce G, Herrod SS, Schmierer K.Mult Scler Relat Disord. 2019 May;30:176-186.
Prof, for those who have failed lemtrada a switch to ocrevus is a common next step though not quick enough to keep secondary auto-immunity in check for some. However, what about the opposite switch? B-cells can take a long time to repopulate after ocrelizumab. If lemtrada was initiated 6 months after the last infusion, does this create a window for the regulatory t-cells to repopulate whilst b-cells are slowly doing the same i.e. preventing the ‘overshoot’ that you have identified as an issue. Also, where does this leave a patient in terms of vulnerability to Covid. Ocrelizumabers are relying on producing t-cell response to vaccines / the virus but if they are wiped out by lemtrada, do you become a sitting duck?
A couple of questions if you don’t mind:
How does all the depressing news regarding ocrevus explain someone having a strong positive spike protein antibody response to the Pfizer vaccine when on ocrevus? I was 9 months post-infusion at the time of my vaccine.
And then – if I have a positive response to the vaccine as I do, am I ok to restart my ocrevus or will it wipe my response? I’m aware we don’t know how long COVID antibodies actually last in anyone anyway, but that’s not my question).
Thanks. I look forward to the T results in the hope I will have some of those to back up my spike antibodies too… 🙏🏼
“I was 9 months post-infusion at the time of my vaccine.”
And so enough of your B cells repopulated in that time to allow a response to the vaccine. Simple as that.
Assuming you have a functioning pool of responding plasma cells to the spike protein, which sounds like you do, then these will not be affected by anti-CD20 as they do not express it and are sequestered in the bone marrow.
Thank you for the reply MD2. Glad I delayed my infusion in the end.
If you look at the Israeli data delay less than 5 months and few converters delay more than 5 months more converters
Does this mean that ocrevus and cladribine are more alike so that it lends itself to immune reconstitution?
yes
The protocol for OCR is standard 600mm per dose, with RTX dosing practitioners may make different decisions. What is the equivalent dosage of RTX to 600mm OCR? Also how much OCR/RTX per dose would be too much for a 50kg person? What are the potential side effects of taking too much OCR/RTX in one infusion?
Has Prof G been glugging the T cell mafia Kool-Aid, I wonder?
🙂
At least Kool-Aid tastes good, which is better than suffering from a widening B-cell mafia induced scotoma 😉
It is now very clear that the majority of B-cell depleted patients with MS continue to smoulder away with worsening disability and accelerated brain atrophy rates. Is this compatible with a treatment response? Or is the B-cell hypothesis simply creating a sense of false security by stopping relapses and focal MRI activity, but doing nothing to address the real MS? Not to mention the emerging safety signal associated with chronic B-cell depletion.
A number of recent posts, plus covid have no doubt led to a number of patients on B-cell depleters to pursue alternative treatment options – Alem, HSCT specifically. From what i can gather, this is not a commonly treaded path. I think i had seen a comment previously that the transfer from Ocrevus to HSCT is one of the least complicated but what about Ocrevus to Alemtuzumab? is there any advantage in having B-cells at a depleted level when initiating this treatment given the issues with potential overshoot?
Very interested in this point. Would it potentially be like derisked alemtuzumab if the anti cd20 was given before?
Might be easier to get than anti cd20 afterwards…
Will the real MS please stand, please stand up………………..boom chicka boom 😉
Mouse doc has been agnaist this t cell expressing cd 20 has a reason for treatment response in patients for years
Will he be convinced this time?
Let’s face it anti-CD20 therapy, which targets B-cell and a proportion of T-cells, is not really effective against smouldering MS. Unlike HSCT/Alemtuzumab than bazookas both B-cells and T-cells. Drawing a Venn diagram what is unique to HSCT/Alemtuzumab is the remainder of the T-cells. My money is on the latter as the treatment target. I suspect B-cells are involved, possibly as a peripheral antigen-presenting cell or as the peripheral reservoir for EBV.
Is it possible to take Alemtuzumab as a third line treatment after failed treatment with Copaxone and Cladribine?
I am not sure why not but I am not a neuro
For a pwMS on Ocrevus whose serological test has shown some immune response, but weak, to the mRNA vaccine (in terms of IgA and IgG), would you recommend a second COVID-19 vaccine booster (i.e., a third injection), provided that the CD19 count is still low (which would presumably make it safe to wait for a response to the third vaccine injection before getting the next infusion), and provided the local supply of mRNA vaccines is plentiful?
Is someone on CD20 therapies able to make plasma cells to new infections? Does Alemtuzumab affect existing immunity to past infections? Thank you in advance.