Barts-MS rose-tinted-odometer: ★★ (mid-week sepia = #704214)


In my post on rebound disease activity in a person with secondary progressive MS switching from fingolimod to siponimod, someone asked whether there is any logic in switching DMTs within the class of S1P modulators. Two or three years ago I would have said no, but now I would say yes. There are well defined and clear differences between the two compounds that may explain their different effects as DMTs in people with more advanced or progressive MS (see figure and table below).

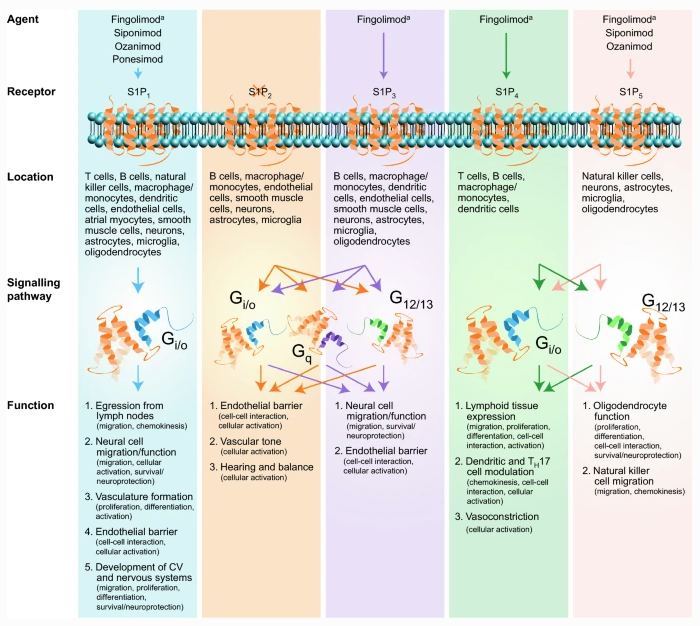
The fact that fingolimod works on a broader spectrum of S1P receptors may explain why it has a greater effect on peripheral immune function, i.e. its action on S1P4 may explain why it disrupts antibody responses to new vaccines. S1P4 plays an important role in the functioning of germinal centres (GCs) in lymph nodes and other secondary lymphoid organs, i.e. so-called follicular T-helper cells use S1P4 for migration signals. If these cells can’t enter the GCs they can’t help B-cells make good antibody responses. I, therefore, predict that vaccine responses in response to the COVID-19 vaccines will be better preserved with siponimod, ozanimod and ponesimod because this new generation of S1P modulators has less or no activity on S1P4 receptors.
Fingolimod needs to be phosphorylated to become active, in comparison siponimod is active already. This may explain why siponimod has greater activity on the S1P5 receptor within the central nervous system (CNS) and explains its greater apparent effects on cells within the central nervous system (CNS). It is clear that when you look at the results of the fingolimod in the PPMS trial there was very little evidence that fingolimod was having any effect on the end-organ, i.e. there was no impact on brain volume loss and no difference across any of the clinical endpoints in the PPMS trial. In comparison, siponimod has a clear CNS signal compared to placebo in subjects with SPMS. Compared to placebo, patients on siponimod have less whole brain, grey matter and thalamic volume loss, preservation of brain tissue integrity on MTR, an MRI marker of myelination, and these effects correlated with better preservation of cognition. On the downside, siponimod was associated with a small but significant risk of seizures, which seems to be more common than with fingolimod in adults with MS.
I have interpreted these results as showing fingolimod as being a more powerful peripheral immunosuppressive therapy but has fewer direct CNS effects. In comparison, siponimod is likely to be less immunosuppressive, but have more direct CNS effects. So based on these differences I think there is a rationale for switching someone on fingolimod to siponimod who has more advanced MS or has transitioned to SPMS. The downside of this switch is that in the NHS you will have to label someone as having SPMS to be able to prescribe siponimod. Using our current criteria SPMS is a one-way street, i.e. once you are labelled as having SPMS you can’t be undiagnosed and converted back to RRMS. As there are no other DMTs currently licensed for SPMS you are therefore theoretically stuck with siponimod. This is why I refer to siponimod as the cul de sac DMT.
The other issue is that to be eligible for siponimod you have to have active SPMS, i.e. relapses or MRI activity (new or enlarging lesions) in the last 2 years. Most people who develop SPMS on fingolimod have inactive SPMS, which means they are not eligible for siponimod. To become eligible under NHS England guidelines you would have to stop fingolimod and hope you develop rebound disease activity that will then allow you to be eligible for siponimod. I have previously stated that I think this is unethical based on our current biological understanding of MS. In any case, once you label someone as having SPMS on fingolimod you are meant to stop their fingolimod in the NHS; the latter is one of the NHS England’s stopping criteria.
So based on the above if you have transitioned to SPMS on fingolimod would you (1) want to switch to siponimod and (2) would you be prepared to stop fingolimod so that your SPMS became active, i.e. developed rebound disease activity?
| Fingolimod | Siponimod |
| MOA: Targets S1P1, S1P3, S1P4 & S1P5 | MOA: Targets S1P1 & S1P5 |
| No baseline pharmacogenomics | Baseline pharmacogenomics (CYP2C9 genotyping)CYP2C9 Genotypes *1/*1, *1/*2, or *2/*2 = 2 mg/dayCYP2C9 Genotypes *1/*3 or *2/*3 = 1 mg /dayModerate CYP2C9 and strong CYP3A4 inducers are not recommended (e.g. rifampin, carbamazepine) |
| First dose monitoring for all patients | First dose monitoring in patients with certain pre-existing cardiac conditions |
| Half life of 6-9 days | Half life of approximately 30 hours |
| Lymphocyte counts progressively return to normal range within 1-2 months of stopping therapy in most patients | Lymphocyte counts return to the normal range within 10 days of stopping therapy in the vast majority (90%) of patients |
| Prodrug – needs to phosphorylated | Active compound no need for activation |
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
If rebound on switching from fingolimod to siponimod is common what does it tell us about the mode of action of these drugs in general and the biology of MS?
It is telling us that S1P3 and S1P4 are potentially important receptors for at least the peripheral effects of fingolimod on MS. Just maybe T-cell help of B-cells in the lymph nodes and secondary lymphoid organs are important for driving MS disease activity.
Prof G,
“Most people who develop SPMS on fingolimod have inactive SPMS”
Isn’t the term “inactive” a misnomer. In other medical conditions “inactive” is a good thing ie the disease is in remission, no more damage is occurring. In MS “inactive” means the opposite – it’s the destruction of brain tissue etc. Are we any nearer to understanding the inactivity and how to treat it?
Inactive MS means NEDA-2 or NEIDA (no evident inflammatory disease activity), i.e. no relapses or focal MRI activity (Gd-enhancing or new/enlarging T2 lesions). You can be NEDA-2 or NEIDA and still be getting worse; the latter is what I call smouldering MS. We need different treatments for smouldering MS. We know the anti-inflammatories such as fingolimod or doing their job because when you stop them inflammatory activity comes back.
Thanks Prof G. I suppose the point I’m trying to make (directed at all neuros, MSologists) is that MS is only being half tackled (for the majority of MSers). Imagine a building company called in to sort out a subsidence problem. They underpin the front of the house, so no more subsidence, but don’t do anything on the back of the house (as they say the reasons for the subsidence are different), so the subsidence continues. I’d argue the job hasn’t been done. Neuros / MSologists need to look at a new 25 year old patient and think “how can I treat this patient so that they will have minimal disability when they are 45, 55, 65?” The problem has been identified – smouldering MS, but the solutions never seem to be delivered.
PS my frustration isn’t targeted at you, but the tens of thousands of MSologists who attend ACTRIMS, ECTRIMS each year who are still focussed on relapses / MRI activity and not the real MS.
See the following that I recorded about SIZOMUS https://youtu.be/vfftVAJfmuM
We are trying. And the CHARIOT-MS study, DoDo study, etc.
Thank you.
If it’s one disease..Isn’t ppms the real smoldering ms…and I don’t
think double doses of rituximab will help.
Please add me to your distribution list.
Click on the three bars on the right side of the blog and subscribe to the blog with your email address and then you will get onto our distribution list 😉
Your cancer colleagues have judt found out anothe MoA for fty-720 🙂
Aging decreases T-cell survival and function.
Aging stress induces mitophagy in T-cells.
Blocking certain ceramide molecules improves the anti-tumor function of aging T-cells.
“What this tells us is that ceramides need to be carefully controlled in a cancer setting,” said Ogretmen. This is particularly important because there are several FDA-approved drugs, such as FTY720 for multiple sclerosis, that increase ceramide signaling. Systemic increase of ceramide signaling in cancer patients may be harmful because it weakens the anti-cancer function of the patient’s immune system, he said
Could pwms on Fingolimod be at an increase risk for cancer?
https://medicalxpress.com/news/2021-06-aging-impairs-anti-tumor-t-cell-response.html