Barts-MS rose-tinted-odometer: ★★★ (a dark blue Saturday; a chastised weekend warrior #00008b )

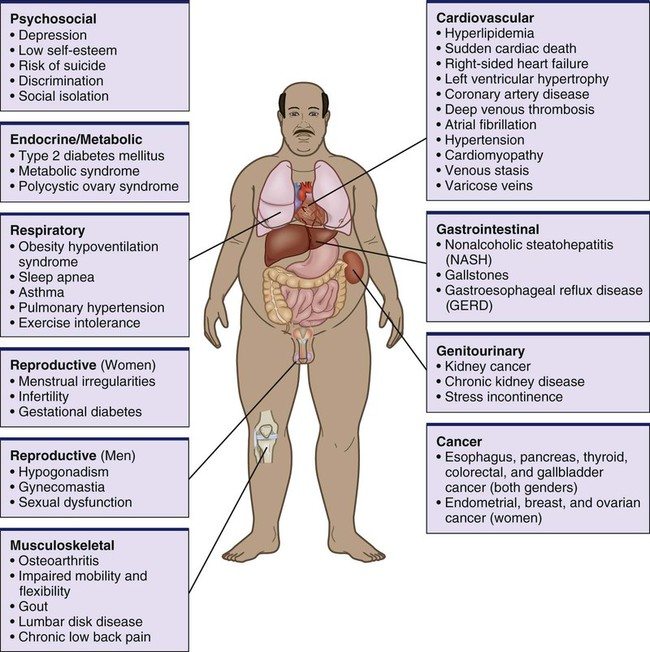
I was accused this week by some commentators on social media for blaming, and by implication shaming, people with MS about lifestyle factors that may impact the long term outcome of their MS. One person said, “stop pushing ‘lifestyle changes’ code for lose weight on people as a fix. It’s insulting and belittling”. In fact, this is incorrect. My dietary recommendations (caloric restriction, intermittent fasting and ketogenic diets) are directed at biohacking and using ketosis as a neuroprotective and pro-remyelinating strategy rather than weight loss. Similarly, exercise (aerobic and HIIT) is about inducing changes within the CNS to promote recovery of function and anti-inflammatory effects in the periphery. The fact that these dietary interventions and exercise can lead to, but not necessarily, weight loss is really not that relevant. Saying this obesity is an issue for pwMS in that that there is a lot of evidence that obesity itself impacts MS outcomes and affects the quality of life of pwMS. In addition, obesity is associated with and causes many comorbidities, which in turn impact MS outcomes (see figure below).
So is obesity a disease or a lifestyle choice? Although this would be a good debate for medical philosophers I am firmly in the camp that at a population level obesity is a metabolic disease that needs to be treated. However, it is up to individuals to choose whether or not they want their obesity treated, in the same way, they have the right to have their MS treated or not.
Some people with MS may not agree with me and hence choose not to have their obesity treated. In these people, obesity is a lifestyle choice and they are presumably well-informed and comfortable with the consequences of being obese. In this situation, who am I to interfere? However, I still feel I have a responsibility to ask the question about the problem?
Because of the sensitive issue of fat-shaming, it is important to open the discussion about weight in a respectful and non-judgmental way. You will be more open to talk about it and seek help if you feel respected. Before asking patients if they wish to discuss their weight, I mention the impact being overweight can have on MS and general health. I usually bundle the weight issue with a discussion about general health and wellbeing. I use the term weight or BMI, which people prefer to the terms such as obesity, obese, fat, excess fat and being overweight. I also cognizant about cultural differences, for example, in certain cultures being overweight is still viewed as a sign of being healthy and/or affluent.
So as a neurologist who manages people with MS should I ignore lifestyle issues such as smoking, alcohol misuse, poor diet, obesity, sedentary behaviour? Maybe this should be left to the GP or family doctor? What does your neurologist do? Another commentator made the point that as I don’t have MS, i.e. have a lived experience of what it is really like to have MS, I shouldn’t expect pwMS to self-manage aspects of their disease such as lifestyle factors. Do you agree?
Please note weight also swings both ways. I have numerous patients who are too thin. Some have eating disorders, others caloric restrict too much to treat their MS, others don’t eat to avoid food coma and others may have a systemic disease associated with loss of weight that needs to be diagnosed and managed. Being too thin is also associated with poor health outcomes. So asking about weight is very relevant to the holistic management of MS.
Please note that over the last 20 years the dogma that obesity is due to ‘too many calories in (overeating) and too few calories out (too little exercise)’ has been debunked. Not all calories are made equal, i.e. not all calorific foods are obesogenic. Obesity is a metabolic or endocrine disorder and there are well-established ways to treat obesity. The corollary is also true, there are well-established ways to become obese. So if you have concerns about your weight, be it that you are underweight or overweight please discuss it with your HCP.
Mendizabal et al. Comorbid disease drives short-term hospitalization outcomes in patients with multiple sclerosis. Neurol Clin Pract . 2020 Jun;10(3):255-264.
Objective: Readmission is used as a quality indicator and is the primary target outcome for disease-modifying therapy (DMT) for multiple sclerosis (MS). However, data on readmissions for patients with MS are limited.
Methods: Using the US Nationwide Readmissions Database, we performed a retrospective cohort study of adults hospitalized for MS in 2014. Primary study outcomes were within 30- and 90-day readmissions. Descriptive analyses compared patient, clinical, and hospital variables readmission status. Multivariable logistic regression models estimated the associations between these variables and readmission.
Results: Of 16,629 individuals meeting the study criteria, most were women (73.7%), aged 35-54 years (48.0%), and Medicare program participants (36.8%). In total, 49.7% of inpatients with MS had 1-2 comorbid medical conditions and 23.7% had 3 or more. Having 3 or more comorbidity conditions associated with increased adjusted odds of the 30-day readmission (adjusted odds ratio [AOR] 1.92, 1.34-2.74). Anemia (AOR 1.62, 1.22-2.14), rheumatoid arthritis/collagen vascular diseases (AOR 2.20, 1.45-3.33), congestive heart failure (AOR 2.43, 1.39-4.24), chronic pulmonary disease (AOR 1.35, 1.02-1.78), diabetes with complications (AOR 2.27, 1.45-3.56), hypertension (AOR 1.25, 1.03-1.53), obesity (AOR 1.35, 1.05-1.73), and renal failure (AOR 1.68, 1.06-2.67) were associated with the 30-day readmission. Medicare insurance and nonroutine discharge were also associated with readmission, whereas patient characteristics (sex, age, and socioeconomic status) were not. The most frequent (26.7%) reason for readmission was multiple sclerosis. Ninety-day analyses produced similar findings.
Conclusions: Comorbid diseases were associated with the readmission for persons with multiple sclerosis. Evaluations of the real-world effectiveness for DMTs in reducing hospitalizations in patients with MS may need to consider comorbid disease burden and management.
Stenberg et al. Bariatric and metabolic surgery in patients with morbid obesity and multiple sclerosis – a nationwide, matched cohort study. Surg Obes Relat Dis. 2021 Jun;17(6):1108-1114.
Background: Despite an association between obesity and multiple sclerosis (MS), very little is known regarding the safety and efficacy outcomes for patients with MS and severe obesity undergoing metabolic surgery.
Objectives: The aim of the present study was to evaluate early complications and efficacy outcomes of metabolic surgery in patients with severe obesity and MS.
Setting: Nationwide, Sweden.
Methods: In this, matched cohort study, 196 patients with an MS diagnosis in the Swedish MS register who were undergoing metabolic surgery (gastric bypass or sleeve gastrectomy) with a registration in the Scandinavian Obesity Surgery Registry (SOReg) were matched 1:10 with a control group without MS diagnosis from the SOReg. A 2-stage matching procedure was used (exact match by surgical method, followed by propensity Score matching, including age, sex, preoperative BMI, surgical center, surgical access, year of surgery, hypertension, diabetes, sleep apnea, and dyslipidemia).
Results: Weight loss at 2 years after surgery was similar for patients with MS and controls (total weight loss 31.6 ± 9.1 versus 31.8 ± 9.2, P = .735). No significant differences were seen in either the overall postoperative complication rate (7.9% versus 7.2%, P = .778), or serious postoperative complications (3.7% versus 2.8%, P = .430). All aspects of health-related quality of life (HRQoL) improved in both groups but less so for the physical aspects of HRQoL in patients with MS.
Conclusion: Metabolic surgery is a safe and efficient treatment for severe obesity in patients with MS, and it leads to subsequent improvements in HRQoL. Further studies addressing the effects of metabolic surgery on MS-related symptoms are needed.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.
I really appreciate you listening to those of us pwMS who are carrying extra weight. I think it should be part of a lifestyle discussion, hopefully Primary Care Doctor can help. My PCP put me on Ozempic and I can’t believe I lost 40 pounds and my numbers (Hgb A1C now normal, vital signs better). I told her, does it make me eat smaller portions? Get full faster? She said Yes. It does. I eat about half as much and then I’m Full. Before Ozempic I felt never hungry and never full. I would say Hereditary + Depression era parents who understood hunger. Do you ever look at a patient with a Normal weight as having some other invisible flaw or self destructive habits? Like bulimia? Yes, you touched a nerve. Yes, you can explain the benefits. Obesity Surgery, however doesn’t fix the problem-The patient still wants to eat-no off switch. It’s tough.
A neurology consultation is a) so precious to the patient b) so short c) so infrequent that perhaps it’s unrealistic for all parties to imagine it will be wholly satisfactory. For the neuro it must be a question of juggling priorities, for the patient the only chance to have a say. I know the approach to MS should be multi-factoriaI and I think that this should be spelled out very clearly by the neuro, so that the patient is aware of the limitations of a neuro consultation. Surely the lifestyle factors are so important that they can’t be ‘assumed’ to be understood but equally the neuro isn’t the best person to go into detail about exercise regimes, diet etc. within a time-limited annual appointment. Patients need an initial input, backed up with factsheets/research findings, on HOW lifestyle affects MS. I don’t mean the general NHS Healthy Living stuff – it needs to be MS-specific, e.g. exactly how and why co-morbidities can hasten progression, effect of poor sleep on symptoms. Then maybe all this screened via questionnaire at nurse or neuro appointments so it assumes an importance parallel to discussion on drugs. Maybe this happens already, but when I heard a version of healthy living advice when I was diagnosed, it didn’t really make an impact because the connection was not direct enough. We’re all swamped with healthy living stuff from media, NHS, supermarkets etc: to someone trying to get their head round MS hearing more of the same, especially if it’s in the last few minutes of their most important appointment of the year is not going to cut it.
‘Fat Shaming’ is an excuse created by the PC brigade to prevent people (including doctors) calling a spade a spade. Sedentary lifestyles and overeating are the reasons we are now in an obesity epidemic. I recall going to the US some 25 years ago, visiting a Levi jeans shop, and seeing men’s jeans up to 56” waist. 25 years on a the U.K. has caught up. Adverts go out of their way showing overweight people declaring that they are comfortable this way. Here’s an extract from the Diabetes U.K. website:
“obesity is believed to account for 80-85% of the risk of developing type 2 diabetes, while recent research suggests that obese people are up to 80 times more likely to develop type 2 diabetes than those with a BMI of less than 22.”
“The life expectancy on average now is reduced by:
Up to 10 years for people with Type 2 diabetes”
Being overweight / obese brings a host of health conditions. Being Fat and Fit is fakery at its best. Doctors need to be straight talking with their patients. Too much time trying to find excuses for gluttony and sloth.
Well said.
The bottom line is a lot of people are lazy. I’m not saying all fat people are lazy, far from it, a lot of people in general population are lazy and won’t / don’t help themselves.
Dieting is hard, if you diet to hard it just doesn’t work people give up and fail. You’ve got to educate yourself.
Personally I don’t think the food pyramid across the western world is the way. To many carbs and not enough healthy fats.
– fatty fish
– avacados
– walnuts
– flaxseed oil
– olive oil and olives
-omega 3s
Fats are branded as the enemy. There not!! It’s the type of fat and what you eat it with.
The first step for any diet in my option would be to totally eliminate sugar with the exception of low carb fruits in small amount such as berries and ELIMINATE PROCESSED FOOD and DRINKS!!!
Spike your insulin and your body stores fat. Simple carbs and sugars spike your insulin levels, and In turn over time causing insulin resistance in cells, not what you want.
Patients rightfully demand access to the best treatments and therapies (and disability if needed). And we should be a lot more aggressive with early HE therapies in almost all locations.
BUT: As a tax payer footing the bill for all of that I expect them to do their share in return. Not all of the above mentioned things are applicable/feasible for everyone (I for one can’t really do keto-diet/IF as much as I’d like as I am borderline underweight as it is and covid sure threw a spanner in my exercise regime) but just declaring defeat and refusing to take any responsibility at all for lifestyle is not acceptable – especially not early in disease course.
While I agree with Kay above, I do appreciate the neurologist, with whom most of us have an ongoing relationship, considering our MS within the framework of our health and lifestyle generally. I do think that given smoking etc have a known impact on our disease that the neurologist would not be doing their job if they didn’t talk to us about such things and suggest paying attention to certain factors which might be making our condition worse. However, beyond that, I think it is then over to us to make the effort and get the support where necessary, probably from our GPs. The fact remains if people don’t know the link between lifestyle and MS issues then they can’t begin to make changes at all if warranted. It would also be good if GPs and neurologists could work in a joined up way with their shared patients. It feels a bit lame telling my GP that the neurologist advised something or other or suggested it might be helpful – they haven’t heard it themselves and only have the patient’s word for it. But maybe that is done in some places and in some situations. Can imagine it would take a lot of organising and everyone is already very stretched.
One important aspect is the quality of the nutrition advice that clinicians give if they choose, or feel compelled, to give any at all.
The low refined-carbs message is creeping in found the more enlightened edges, but the official discourse remains dominated by the old low fat/very low saturated fat/healthywholegrains/starchy veg/eat less/move more messages that are just not helpful to a person with MS already in metabolic trouble. What can we do to change this?
I totally see your point of view. I spent many years, pre diagnosis, addressing what was considered lifestyle or stress related issues. However, it was the MS that was causing all these symptoms. It is MS that makes it difficult to address issues related to food intake and movement. In my 30’s and 40’s I used to run but could never seem to improve. I kept getting slower and in the summer months I simply could not move like I could in the cooler months. Today in my 50’s after finally getting a diagnosis in my late 40’ s I can walk and with walking poles I can walk fast enough to raise my heart rate. However, doing so no longer has the rejuvenating effect that exercise used to have. Thus not being able to do other activities like make healthy food or take care of household tasks and work. This spiral can lead to feelings of sadness, grief and frustration etc. So I can understand why pwMS feel triggered by these statements you are making. While true, many of us don’t have the kind of support to address the variables that create the barriers to better health. When I was able to work I was a community health social worker helping people, like me, adjust to their illness. So I can see both sides of the fence as I have been on both sides. I have never heard a health care professional tell me there was any medical treatment for obesity. So the information you have is not widespread. We have a long way to go still in providing comprehensive care to pwMS and other mobility related chronic diseases.
Having watched the bbc documentary ‘What are we feeding our kids?’ I now comprehend the extent to which we all consume ultra-processed foods, even those of us who watch our diet
It was very striking when the consultant Rachel Batterham, who’s an expert in obesity, says that even she’s realised the portion she’s feeding her children is higher than she’d like – because products such as wholemeal sliced bread are in fact highly processed.
She adds that there’s actually been very little research into the effects of the diet we all now consume and talks about this in respect to the brain.
The finger was clearly pointed at the food industry and not at us mere human beings, due to the onslaught of food we consume being engineered to engender things such as the bliss point – guaranteed to make us want to consume more and then to make it all available below the cost of fresh food: it costs twice as much to get 100 calories this way than it does from ready prepared food.
The killer moment after the guy from the Food and Drinks Federation gives the line about people need to make good choices, is when he’s asked which is the priority: public health or profit he replies: ‘the priority is profit’
This therefore needs as many people as possible to heed the oft repeated advise for the likes of ProfG, coz clearly we’ve all an uphill battle and jeez do we all need to begin to push back against the food industry and not allow the line about individual responsibility/people are being weak-willed etc to keep being pedalled!
When I was first diagnosed my neurologist told me to try to eat healthy balanced meals, complex carbohydrates, etc.. he told me to lose weight of I could and to try to exercise five times a week even if it was something very simple. He was a well known neurologist getting ready to retire and these were oart igmf his words of wisdom. I am forever thankful that he did. I changed my lifestyle and my priorities and over 6 years or so since then lost 40 pounds. He was very direct and mattervof fact about it. No shaming or fear tactics. I think you are totally doing the right thing.
How about measuring postprandial responses in MS?
New Study Findings: The Surprising Impact of Eating on Your Inflammation Levels https://youtu.be/ol6wTjj7Y18
Human postprandial responses to food and potential for precision nutrition.
Berry SE, Valdes AM, Drew DA, Asnicar F, Mazidi M, Wolf J, Capdevila J, Hadjigeorgiou G, Davies R, Al Khatib H, Bonnett C, Ganesh S, Bakker E, Hart D, Mangino M, Merino J, Linenberg I, Wyatt P, Ordovas JM, Gardner CD, Delahanty LM, Chan AT, Segata N, Franks PW, Spector TD.
Nat Med. 2020 Jun;26(6):964-973. doi: 10.1038/s41591-020-0934-0. Epub 2020 Jun 11.
PMID: 32528151
This is the latest study: doi: https://doi.org/10.1093/ajcn/nqab132
Of course pwMS should self-manage lifestyle factors. If we educate ourselves about how to manage our disease and take action, that gives us back some sense of control over something that at times seems uncontrollable.
I have to say though that my GP doesn’t really approve of my lifestyle. My plant based + fish diet is something he sees as dangerous, despite my blood tests coming back good for b12, iron, folate, vitamin D, and everything else except I have high MCV (investigated and nothing to cause alarm, hence knowing my levels are ok for everything else!).
I run several times a week and took up cycling during lockdown, for transportation rather than exercise but I’ve been cycling 6 miles and back to my office 1-2 times a week. At my mother’s prompting I asked my consultant “should I really be doing all those ultras?” (her words) and he said “I can think of no neurological reason why you shouldn’t”
I don’t really feel like I trust my GP to have these conversations. But my consultant, sure. I met with the nurse consultant at my hospital once too and she was fab, told me I’m doing everything right.
I for one really appreciate your observations on biohacking/lifestyle choices that could possibly help improve health for PwMS. It is useful to hear from someone who is knowledgeable about the whole sphere, if that makes sense, and has time to devote to it as both part of their work but also outside of work. I don’t have the time to survey all the info available to keep up to date with this myself.
This post, and the ‘ask not’ post, leads me to wonder whether there’s a case for developing some form of online [therefore easily updatable] information repository/manual for people who want to keep up to date with what they can do for themselves, maybe share tips and experiences?
As you often ask: What do you think?
That thought struck my mind reading those articles, too.