Barts-MS rose-tinted-odometer: ZERO-★’S (Black Tuesday – a tear for my beloved country #000000)
As you are aware by now I am a proponent of flipping the pyramid and using high-efficacy DMTs first-line including immune-reconstitution therapies (IRTs) such as alemtuzumab and AHSCT. I justify the latter two options based on the fact that given sufficient time the vast majority of pwMS will become disabled and the real cost of MS to people with MS cannot be underestimated; loss of employment, poor relationships, cognitive impairment, fatigue, depression, anxiety, etc. I think you get the gist; MS is a bad disease.
Alemtuzumab and HSCT are the two standout treatment options that offer pwMS the best chances of long-term remission and in some pwMS it may offer a cure. What impresses me about these two options is their impact on the end-organ, i.e. brain volume loss. After rebaselining at 12 months, pwMS treated with these two options lose brain volume on average at a rate that is within the normal range for age. The other DMTs don’t do this. The downside is that these two treatment options come with more risks. These two real-world studies below report 2 deaths out of 121 (2.5%) alemtuzumab-treated patients in Finland and 3 out of 120 HSCT-treated patients in London. Would you be willing to take these chances of dying to treat your MS with the potential for long term remission, possibly a cure and to protect your most precious end-organ the brain?
Background: Alemtuzumab is an effective disease-modifying therapy (DMT) for highly active multiple sclerosis (MS). However, safety concerns limit its use in clinical practice.
Objectives: To evaluate the safety of alemtuzumab in a nationwide cohort of Finnish MS patients.
Methods: In this retrospective case series study, we analyzed the data of all but two MS patients who had received alemtuzumab in Finland until 2019. Data were systematically collected from patient files.
Results: Altogether 121 patients were identified, most of whom had received previous DMTs (82.6%). Median follow-up time after treatment initiation was 30.3 months and exceeded 24 months in 78 patients. Infusion-associated reactions (IARs) were observed in 84.3%, 57.3%, and 57.1% of patients during alemtuzumab courses 1-3, respectively. Serious adverse events (SAEs) were observed in 32.2% of patients, serious IARs in 12.4% of patients, and SAEs other than IARs in 23.1% of patients. Autoimmune adverse events were observed in 30.6% of patients. One patient died of hemophagocytic lymphohistiocytosis, and one patient died of pneumonia. A previously unreported case of thrombotic thrombocytopenic purpura was documented.
Conclusions: SAEs were more frequent in the present cohort than in previous studies. Even though alemtuzumab is a highly effective therapy for MS, vigorous monitoring with a long enough follow-up time is advised.
Objective: to examine outcomes in people with multiple sclerosis (PwMS) treated with autologous hematopoietic stem cell transplantation (AHSCT) in a real-world setting.
Methods: retrospective cohort study on PwMS treated with AHSCT at two centers in London, UK, consecutively between 2012 and 2019 who had ≥ 6 months of follow-up or died at any time. Primary outcomes were survival free of MS relapses, MRI new lesions and worsening of expanded disability status scale (EDSS). Adverse events rates were also examined.
Results: the cohort includes 120 PwMS; 52% had progressive MS (primary or secondary) and 48% had relapsing-remitting MS (RRMS). At baseline, the median expanded disability status scale (EDSS) was 6.0; 90% of the evaluable cases showed MRI activity in the 12 months preceding AHSCT. Median follow-up after AHSCT was 21 months (range 6-85). MS relapse-free survival was 93% at 2 years and 87% at 4 years after AHSCT. No new MRI lesions were detected in 90% of subjects at 2 years and 85% at 4 years. EDSS progression-free survival (PFS) was 75% at 2 years and 65% at 4 years. EBV reactivation and monoclonal paraproteinemia were associated with worse PFS. There were 3 transplant-related deaths within 100 days (2.5%), all following fluid overload and cardiac or respiratory failure.
Conclusions: efficacy outcomes of AHSCT in this real-world cohort are similar to those reported in more stringently selected clinical trial populations, although the risks may be higher.
Classification of evidence: this study is rated Class IV because of the uncontrolled, open-label design.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.
Barts-MS rose-tinted-odometer: ★★★★★ (aquamarine on a very rainy Friday in London, #00FFBF)
I recently had a patient of mine who has been desperate to be treated with alemtuzumab actually ask if he can change his mind and rather be referred for AHSCT (autologous hematopoietic stem cell transplantation). Why? Because the chances of being put into long term remission, and hence potentially being cured of having MS, seems to be much higher with AHSCT. This particular patient has no concerns about the risks associated with alemtuzumab or AHSCT. The most important concern on his radar is his long term outcome. He wants a healthy brain when he gets older.
This is why this most recent paper on the long term outcome of Italian patients who received AHSCT adds to the mounting evidence base of the effectiveness of AHSCT. In patients with relapsing-remitting treated with AHSCT, MS 86% and 71% were free of disability worsening at 5 and 10 years, respectively. These figures for patients with progressive MS were 71% and 57% at 5 and 10 years, respectively.
The results are less impressive when using NEDA-3 status, i.e. no relapses, MRI activity or disability progression. For patients with RRMS, probabilities of achieving NEDA3 status were 62% at 5 years and 41% at 10 years, respectively. However, and importantly, in the subgroup of patients with RRMS who underwent AHSCT with the BEAM+ATG conditioning protocol, which is more aggressive, NEDA-3 status was achieved in 68% and 55% of subjects at 5 and 10 years, respectively.
In subjects with progressive MS, NEDA-3 status was only achieved 51% and 37% of subjects at 5 and 10 years, respectively.
On average, disability scores improved in relapsing-remitting subjects and got worse in subjects with progressive disease, which implies that AHSCT does not stop smouldering disease. However, almost all subjects had failed one or more DMTs prior to AHSCT. The latter is important. The average EDSS was ~6.0 and most patients had a disease duration of longer than 10 years. This makes me wonder how better the results would be if AHSCT was done earlier in the course of MS, i.e. before too much damage to the brain and spinal cord had accumulated. This is why we really need to test AHSCT as first-line therapy in MS. Could AHSCT done early stop/reverse or prevent the establishment of smouldering disease? In other words, does AHSCT cure people from having MS? This is why a trial of AHSCT in very early MS, i.e. as a first-line treatment, is a no-brainer to me.
Please note that three deaths occurred due to AHSCT, which was 1.4% of the entire study population.
The take home messages are:
AHSCT is the most effective DMT we have for treating MS.
RRMS responds better to AHSCT than progressive MS.
BEAM+ATG conditioning protocol is superior to cyclophosphamide-based protocols.
Mortality remains relatively high with AHSCT.
The results would be much better than this if patients had had AHSCT earlier in the course of their disease.
I was criticised yesterday for suggesting lifestyle changes to pwMS when I had no idea what it was like to have MS. It was implied that unless you have lived with MS, i.e. the lived experience, I shouldn’t be making any lifestyle recommendations to pwMS particularly around weight loss and diet. What I can say is that I have treated and followed thousands of people with MS and I know enough that if I had MS I would have no hesitation in wanting to be treated first-line with AHSCT or alemtuzumab and to manage all the lifestyle issues I referred to in my post ‘ASK NOT‘.
What underpins my decision to be treated with alemtuzumab and AHSCT first-line is the data missing from this paper on the end-organ; both of these treatments will on average normalise brain volume loss in treated subjects. In other words, these treatments are on top of the ladder when it comes to preventing end-organ damage. The downside of AHSCT is that the brain takes a significant neurotoxicity hit from the chemotherapy with accelerated brain volume loss in year one. In addition, there is also the high, but delayed secondary malignancy risk and high mortality risk associated with AHSCT that needs to be taken into account. Therefore, alemtuzumab probably wins out on safety as a potential first-line therapy. Please remember being treated with alemtuzumab does not exclude you from being treated with AHSCT at a later stage.
Objective: To determine whether autologous hematopoietic stem cell transplantation (aHSCT) is able to induce durable disease remission in people with multiple sclerosis (MS), we analyzed the long-term outcomes after transplant in a large cohort of MS patients.
Methods: To be included, a minimum data set (consisting of age, MS phenotype, EDSS at baseline, information on transplant technology and at least 1 follow-up visit after transplant) was required.
Results: 210 patients were included [relapsing-remitting (RR)MS=122(58%)]. Median baseline EDSS was 6(1-9), mean follow-up was 6.2(±5.0) years. Among RRMS patients, disability worsening-free survival (95%CI) was 85.5%(76.9-94.1%) at 5 years and 71.3%(57.8-84.8%) at 10 years. In patients with progressive MS, disability worsening-free survival was 71.0%(59.4-82.6%) and 57.2%(41.8-72.7%) at 5 and 10 years, respectively. In RRMS patients, EDSS significantly reduced after aHSCT [p=0.001; mean EDSS change per year -0.09 (95%CI=-0.15 to -0.04%)]. In RRMS patients, the use of the BEAM+ATG conditioning protocol was independently associated with a reduced risk of NEDA-3 failure [HR=0.27(0.14-0.50), p<0.001]. Three patients died within 100-days from aHSCT (1.4%); no deaths occurred in patients transplanted after 2007.
Conclusions: aHSCT prevents disability worsening in the majority of patients and induces durable improvement in disability in patients with RRMS. The BEAM+ATG conditioning protocol is associated with a more pronounced suppression of clinical relapses and MRI inflammatory activity.
Classification of evidence: This study provides Class IV evidence that for people with MS, aHSCT induces durable disease remission in most patients.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.
Side of the fence: used to refer to either of the opposing positions or interests involved in a particular situation.
Status quo: the current situation; the way things are now. The MS community, i.e. patients and HCPs are content with the status quo and aren’t looking for a change.
NEDA: no evident MS disease activity
The question you need to ask yourself is which side of the fence are you on? MS is a focal inflammatory disease of the central nervous system vs. MS is a smouldering disease process and focal inflammatory events are in response to what is causing the disease. If you favour the former you will be happy with being NEDA-2, i.e. having no relapses or new focal inflammatory lesions. If you are in the latter camp you will want to focus on end-organ damage and preserving your brain and spinal cord volume for old age.
The wider MS community seems to prefer the current dogma and status quo; i.e. that MS is a focal inflammatory disease and that everything we see can be explained by relapses and focal MRI activity. I think this is wrong and have argued this from not only a scientific point of view but also from a philosophical one.
Deciding which side of the fence you are on may make an enormous difference to your outcome. It is clear that not all DMTs are made equal when it comes to preserving brain volume and hence brain reserve.
Did you know that pwMS lose brain volume at a 2-7x faster rate than age-matched controls from the general population? Accelerated brain volume loss predicts and is strongly associated with cognitive impairment and long term disability. The following picture shows you just how much brain someone with MS can lose over an 18 month period.
If we moved our treatment target to go beyond NEDA to focus on protecting the end-organ so that pwMS may have a brain that is in good enough condition to withstand the ageing process in later life I suspect the treatment landscape would change dramatically. To achieve this we need to diagnose MS and treat it early and effectively and in many cases, we need to flip the pyramid and use high efficacy therapies at the beginning, in particular agent such as alemtuzumab and AHSCT, which have been shown to protect the end-organ better than other DMTs.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
The one good thing about thinking aloud is that your colleagues’ chip in and provide feedback. Case 2 from my ‘ethical quandary post‘ is generating an important debate about whether to support this patient’s decision to switch therapy or not.
As a reminder, this is the 40-year old woman who started natalizumab as a first-line therapy 11 years ago after presenting with two disabling relapses in a four-month period. She has done exceptionally well on natalizumab, i.e. she is NEDA-3 (no relapses, no MRI activity and no change in her EDSS). In fact, her original disabilities from the two relapses recovered. At present she is fully functional, working full-time and very active physically. For example, she plays competitive tennis in her local sports club and ran the London marathon 2 years ago. Her current EDSS is 1.0.
The problem is that her serial annual MRI studies demonstrate that she has progressive macroscopic (visible by the naked eye) brain volume loss. Being an intelligent woman and a self-taught MS expert she knows this is a poor prognostic sign and she wants to stop natalizumab and have HSCT or alemtuzumab. She is aware from reading The MS-Blog (formerly the Barts-MS blog) that alemtuzumab and HSCT have a greater impact than natalizumab on end-organ damage or brain volume loss. After HSCT and alemtuzumab treatment brain volume loss is on average in the normal range (please see BEYOND NEDA).
What I didn’t say to you is that this lady has already made the decision that she wants to be treated with AHSCT, either on the NHS (not possible at present), abroad at one of the reputable private BMT units or in the private sector within the UK. The problem we have is that we have no idea what will happen to her BVL once she makes the switch. I suspect she will have accelerated BVL in the first year post-AHSCT, which is well described and is likely to be due to the neurotoxicity of the chemotherapy. After year-1 the BVL may or may not normalise. We have no idea what happens to the MS brain after being subjected to smouldering MS pathology on natalizumab for a decade.
Fortunately, we do have data from interferon-beta to alemtuzumab switching and, yes, after 2 years of interferon-beta therapy switching to alemtuzumab does normalise BVL. What is clear from the 8-year alemtuzumab follow-up data (see below) is that the rate of brain volume loss is age-dependent. Being in the 35-45 year age group the BVL was 0.13% per annum ((1.51-0.71)/6) on alemtuzumab. When you compare this to the 0.06% per annum in study subjects 18-25 years of age ((1.24-0.87)/6) you realise how important age is in determining treatment effects.
Is this data sufficient to talk this young woman down from her decision to have AHSCT and to go with alemtuzumab? What do you think? If this patient is reading this blog post will it affect your decision?
Another thing this ‘thinking out loud’ exercise has taught me is that having annual BVL measurements on our patients with MS on DMTs could be very helpful. I also think we should ask around to see if we can get a case series of natalizumab to alemtuzumab switchers to see what happens to the trajectory of BVL before, on natalizumab, and after the switch to alemtuzumab. At least then we will have data to inform such difficult decisions.
Background: Alemtuzumab significantly improved clinical and MRI outcomes vs. subcutaneous interferon beta-1a (SC IFNB-1a) in the CARE-MS trials (NCT00530348, NCT00548405), with sustained efficacy in 2 consecutive extensions (NCT00930553, NCT02255656 [TOPAZ]).
Methods: Post hoc analysis of 8-year alemtuzumab efficacy and safety in pooled CARE-MS patients (N=811) stratified by baseline age (≥18 to ≤25, >25 to ≤35, >35 to ≤45, >45 to ≤55 years).
Results: Compared with SC IFNB-1a over 2 years across age cohorts, alemtuzumab lowered annualized relapse rates (ARR; 0.22-0.24 vs. 0.38-0.51), improved or stabilized disability (freedom from 6-month confirmed disability worsening [CDW]: 85%-92% vs. 62%-88%; achievement of 6-month confirmed disability improvement [CDI]: 20%-31% vs. 13%-25%), increased proportions free of MRI disease activity (70%-86% vs. 42%-63% per year), and slowed brain volume loss (BVL; -0.45% to -0.87% vs. -0.50% to -1.39%). Through Year 2, the treatment effect with alemtuzumab did not significantly differ among age groups for ARR (p-interaction=0.6325), 6-month CDW-free (p-interaction=0.4959), 6-month CDI (p-interaction=0.9268), MRI disease activity-free (p-interaction=0.6512), and BVL (p-interaction=0.4970). Alemtuzumab remained effective on outcomes through Year 8 across age groups. Age-related increases in malignancies (≤45 years: 0.9%-2.2% vs. >45 years: 8.1%) and deaths (0%-1.7% vs. 7.0%) were observed. Serious infections also increased from the youngest (5.1%) to oldest (12.8%) age cohorts.
Conclusions: Alemtuzumab had greater efficacy than SC IFNB-1a over 2 years across comparable age groups, with no significant differences between alemtuzumab-treated age groups. Efficacy on relapse, disability, and MRI outcomes continued through Year 8 across age groups. Age-related increases in serious infections, malignancies, and deaths were observed.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
Shortly after leaving Queen Square to take up my current position at Barts and The London Juliet Solomon, a good friend, and one of the research managers who had an office opposite me on the 6th floor of the Institute of Neurology sent me a signed copy of the ‘The Book of Regrets’ she had compiled as a present. She has asked celebrities to write essays on something they had regretted in their lives. The book has become a bestseller with all the proceeds of the sales going to support the National Hospital for Neurology and Neurosurgery. This is the kind of thing Juliet does; she has a very big heart. A mensch!
At the time I thought about what I would write if I was asked to contribute a chapter to the next edition of the book. I am still not sure, but from a professional perspective, my biggest regret is not being more proactive in derisking alemtuzumab as a treatment for MS. It has become clear to me that a small proportion of people with MS (pwMS) who are treated with alemtuzumab and HSCT early in the course of their disease are cured of MS when you use a contemporary definition of an MS cure.
If the infusion reactions, infections and secondary autoimmunity problems went away who would choose anything but alemtuzumab to treat their MS?
Infusion reactions: Can we reduce the infusion reactions of alemtuzumab? Yes, we can. Pre-treating with steroids starting the night before and moving from the intravenous to the subcutaneous route would make infusion reactions minor. So why hasn’t this been done? Money! MS centres/units make lucre out of infusing patients. I have used the subcutaneous route to avoid a second about of steroid-induced psychosis, to avoid steroid-induced metabolic mayhem in a patient with MS and type 1 diabetes and in a patient who developed avascular necrosis of one hip after his first course of alemtuzumab. It was remarkable; there were no major alemtuzumab infusion reactions despite these three patients being steroid-free. The pharmacodynamic data, i.e. the cell depletion data for the IV and SC routes are identical. The main reasons for us not switching all our patients to subcutaneous alemtuzumab was money, resource and inertia. In the recent past, we used to make money for the unit by giving infusions. Fortunately, with NHS block contracts, this perverse incentive has disappeared. Sanofi-Genzyme also provides contract nurses who come in to give the infusions and monitor the patients. If we converted our entire alemtuzumab administration programme to a subcutaneous route the workload would fall on our overworked nurses. Our nursing lead in our daycare unit reminded me of this. REGRET 1 we didn’t covert to sc alemtuzumab.
Secondary autoimmunity: What about preventing or reducing the incidence of secondary autoimmunity?
The immune system has many mechanisms in place to prevent autoimmunity. When you learn how the immune system works it is really quite surprising that autoimmunity is so uncommon. What the immunologists tell us is that there must be a series of underlying biological processes that are causing secondary autoimmunity and if we can work out what these are we can intervene and prevent this complication. This is what Joanne Jones and Alasdair Coles tried to do in Cambridge. Their hypothesis was that because the immune system reboots itself from peripheral memory cells it is more likely to result in an aberrant autoimmune response. They tried rebooting the immune system using more naïve cells from the thymus using the hormone palifermin, which stimulates the thymus to produce more naïve T-cells. Sadly it didn’t work, but at least they tried and they should be congratulated for doing this study.
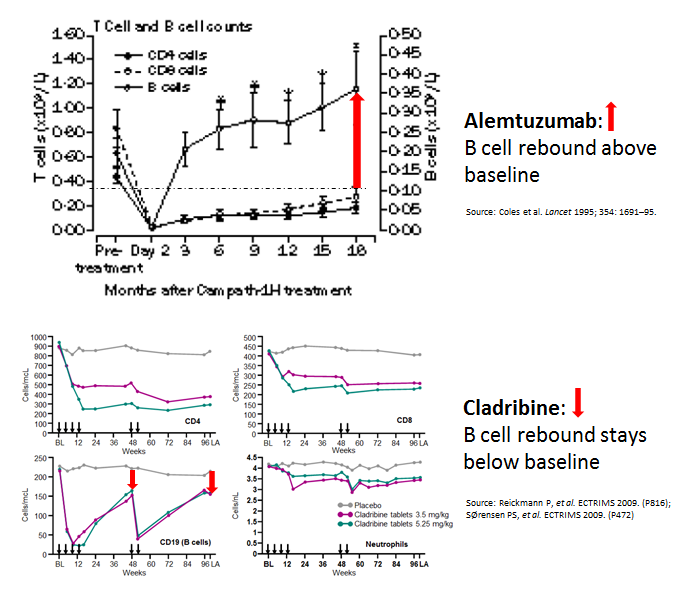
Interestingly, when you compare cladribine, another IRT, with alemtuzumab you can’t help but notice that the B-cell reconstitution profiles are very different. With alemtuzumab, they come back very quickly and overshoot their baseline values. We, and others, have hypothesised that if you change the profile of the B cell reconstitution with a small dose of the B cell depleting antibody rituximab you may be able to prevent this secondary autoimmunity. We are really talking about a very small dose of rituximab, i.e. 10-20mg, just enough to delay B cell reconstitution by 4-6 months. I proposed this concept to Genzyme 8 or 9 years ago, but without data to support the hypothesis they were not keen to support an exploratory study. Why didn’t I push to get this funded from another source? If we had done this study back then we would have had the results by now. Can you imagine how impactful this could be for pwMS if we could prevent secondary autoimmunity post-alemtuzumab? REGRET 2 no doing alemtuzumab-rituximab trial and not setting up an adaptive trial platform for testing multiple strategies to prevent secondary autoimmunity post-alemtuzumab.
Infections: One success story has been the derisking of alemtuzumab-associated infections with prophylactic antibiotics and antivirals, and the proactive approach to baseline infectious disease screening and vaccination. SUCCESS 1 reducing alemtuzumab-associated infections.
Anti-drug antibodies: Another success story has been exposing alemtuzumab’s problems with anti-drug antibodies (ADAs) and the development of an assay to screen for these antibodies. Why use a therapy, at great expense, that is not going to work because of neutralizing anti-drug antibodies. SUCCESS 2, anti-drug antibody screening.
A big problem that emerged was how alemtuzumab was licensed and used in the USA. The FDA has essentially licensed alemtuzumab with hand-cuffs, therefore, alemtuzumab was and is used as the DMT of last resort in the US. This led to it being used in an older more advanced cohort of pwMS who had comorbidities. In this group of patients, a new adverse event profile emerged, particularly vascular complications. This led to a safety review and the license of alemtuzumab’s use was changed and it is now only used infrequently, second or third -line and often in people with more advanced MS. I was personally involved with the original EMA submission; it was a real uphill battle to get alemtuzumab licensed as first-line therapy. Allowing the EMA to change how we use alemtuzumab, i.e. making pwMS have to wait to become eligible for the therapy is a travesty. We, Genzyme and MS community, should have made a more robust argument to the CHMP not to change alemtuzumab’s label. REGRET 3 not allowing alemtuzumab to be used first-line in active MS; it can only be used as a first-line agent in patients with rapidly evolving severe (RES) MS (two disabling attacks in a 12 month period). The problem is that very few patients have RES MS as they tend to be treated now before they have their second disabling relapse.
Finally, my colleagues. Apart from a small group of MSologists, and we know who we are, most MSologists don’t prescribe alemtuzumab. They find the therapy too difficult and risky to use. I have tried to educate and get more of my colleagues to at least offer alemtuzumab as an alternative to HSCT, but to no avail. In the UK, we were all geared up to do a head-2-head study of alemtuzumab vs. AHSCT. However, once ocrelizumab was licensed the MS community said they would not be able to recruit for this trial so it has now been converted into alemtuzumab or ocrelizumab vs. AHSCT trial. In reality, this study is going to be a head-2-head of ocrelizumab vs. AHSCT study. Not getting the wider MS community to understand how effective alemtuzumab is REGRET 4. Instead of success, we have a generation of refuseniks.
The question we need to ask ourselves is do we really want to throw the baby out with the bathwater? We have two, and possibly three, treatment strategies that may cure a minority of pwMS of having MS. Yes, CURE. However, alemtuzumab and HSCT are on the fringe of MS treatments. Why?
I suppose you are asking about the third option. It may be cladribine. The results of the ORACLE trial of cladribine in patients with clinically isolated syndromes (CIS) are quite remarkable. We are trying to recall the patients from the ORACLE study a decade or more later to see how many are still in remission and haven’t converted to MS. The problem we have is that cladribine is not even a treatment option for CIS despite this stunning data, hence we may be denying a large number of people with CIS, a relatively safe immune reconstitution therapy or IRT, that may prevent many of them from developing MS. The downside of this is the depressing fact that many MSologists still don’t treat CIS (see my blog post on watchful waiting).
Alemtuzumab is an anti-CD52 monoclonal antibody with remarkable efficacy in relapsing multiple sclerosis (MS). In clinical trials and off-label use in MS, alemtuzumab has been administered intravenously (IV). Alemtuzumab is approved for chronic lymphoid leukemia as IV. Oncology guidelines recommend alemtuzumab subcutaneous (SC) over IV. There is no report of alemtuzumab SC in MS. We report two patients with highly active relapsing MS who were treated with SC alemtuzumab, had significant improvement and tolerated SC alemtuzumab well without the typical infusion-associated adverse events. SC alemtuzumab in MS warrants further studies as this may enhance patient convenience and minimize infusion-associated adverse events.
Background: Patients who develop relapsing-remitting multiple sclerosis (MS) present with a first clinical demyelinating event. In this double-blind, multicentre, randomised, phase 3 study we investigated the effect of oral cladribine on conversion to clinically definite MS in patients with a first clinical demyelinating event, when given at the same doses shown to be effective in relapsing-remitting MS.
Methods: Between Oct 21, 2008, and Oct 11, 2010, we recruited patients aged 18-55 years, inclusive, from 160 hospitals, private clinics, or treatment centres in 34 countries. Eligible patients had a first clinical demyelinating event within 75 days before screening, at least two clinically silent lesions of at least 3 mm on a T2-weighted brain MRI scan, and an Expanded Disability Status Scale score of 5.0 or lower. Patients with a first clinical demyelinating event ≤75 days before screening were randomly assigned (1:1:1) to receive cladribine tablets at cumulative doses of 5.25 mg/kg or 3.5 mg/kg or placebo. Randomisation was done with a central web-based randomisation system and was stratified by geographic region. Masking was maintained using a two-physician model. The primary endpoint of this 96-week study was time to conversion to clinically definite MS according to the Poser criteria. This study is registered with ClinicalTrials.gov, number NCT00725985.
Findings: Of 903 participants assessed for eligibility, 616 patients received cladribine 5.25 mg/kg (n=204), cladribine 3.5 mg/kg (n=206), or placebo (n=206). At trial termination on Oct 25, 2011, cladribine was associated with a risk reduction versus placebo for time to conversion to clinically definite MS (hazard ratio [HR] for 5.25 mg/kg=0.38, 95% CI 0.25-0.58, p<0.0001; HR for 3.5 mg/kg=0.33, 0.21-0.51, p<0.0001). Adverse events were reported in 165 (81%) patients in the cladribine 5.25 mg/kg group, 168 (82%) patients in the cladribine 3.5 mg/kg group, and 162 (79%) patients in the placebo group. We noted no increase in risk of adverse events with active treatment versus placebo apart from lymphopenia, which was a severe event in 10 (5%) patients in the 5.25 mg/kg group and four (2%) patients in the 3.5 mg/kg group.
Interpretation: Both doses of cladribine significantly delayed MS diagnosis compared with placebo. The safety profile of cladribine was similar to that noted in a trial in patients with relapsing-remitting MS. Further research could clarify the potential effects of oral cladribine treatment in the early stages of MS.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
The two case studies below are creating an ethical quandary in my MS practice. Can you help me please?
Case 1
The first is the 40-year old woman with MS who is NEDA-2 (no evident disease activity) on DMF (Tecfidera) with no documented relapses in the last 4 years and a series of annual MRI scans with no new or enlarging T2 MS lesions. However, there has been a worsening of her disability; increasing bladder problems and a progressive spastic paraparesis (weak legs). Her EDSS has moved from 4.0 to 5.5 in the last three years. She has self-diagnosed herself as having secondary progressive MS and wants to switch to siponimod. Unfortunately, according to the current NICE approval and NHSE guidelines, this patient is ineligible for siponimod because she has inactive MS (NEDA-2).
Do I recommend she stops her DMF so that her MS can reactivate, which will then make her eligible for siponimod? Most MSologists would say yes, mainly because the development of SPMS is one of NHS England’s stopping criteria. The problem I have is we, the patient and I, have no idea how active her MS will become if and when her MS reactivates. For example, she could have a catastrophic spinal relapse that leaves her doubly incontinent and quadriplegic or it may be on the other side of the spectrum, i.e. one or two new asymptomatic MRI lesions on her annual MRI follow-up. If you were in her position would you stop your treatment to develop active MS?
Case 2
The second is the 40-year old woman who started natalizumab as a first-line therapy 11 years ago after presenting with two disabling relapses in a four-month period. She has done exceptionally well on natalizumab, i.e. she is NEDA-3 (no relapses, no MRI activity and no change in her EDSS). In fact, her original disabilities from the two relapses recovered. At present she is fully functional, working full-time and very active physically. For example, she plays competitive tennis in her local sports club and ran the London marathon 2 years ago. Her current EDSS is 1.0.
The problem is that her serial annual MRI studies demonstrate that she has progressive macroscopic (visible by the naked eye) brain volume loss. Being an intelligent woman and a self-taught MS expert she knows this is a poor prognostic sign and she wants to stop natalizumab and have HSCT or alemtuzumab. She is aware from reading The MS-Blog (formerly the Barts-MS blog) that alemtuzumab and HSCT have a greater impact than natalizumab on end-organ damage or brain volume loss. After HSCT and alemtuzumab treatment brain volume loss is on average in the normal range (please see BEYOND NEDA).
Would you allow this patient to switch treatments? Under the current London MS HSCT guidelines she would not be eligible for HSCT as she has not failed natalizumab; please note, progressive brain volume loss is not considered a treatment failure. What about alemtuzumab? Applying the strict NHSE guidelines she would not be eligible for alemtuzumab as her MS is inactive at present. However, one could argue that we need to go back to 2010 when she started natalizumab and ask ourselves now would she have been eligible back then if alemtuzumab had been available? The answer is yes as she had what we call rapidly evolving severe MS; in 2021 someone with rapidly evolving severe MS could be treated with alemtuzumab first-line. Should we apply treatment criteria retrospectively?
This patient is JCV negative. If, however, she seroconverted to being JCV positive it would be easier to justify to NHS England for the switch to alemtuzumab, i.e. NHSE guidelines support the principle of derisking PML. The one thing I can’t tell this patient is whether or not alemtuzumab or HSCT will have an impact on her brain volume loss as we simply don’t have the data from a cohort of patients making the switch from natalizumab to alemtuzumab 10+ years into their disease. In other words will the smouldering or real MS that causes the accelerated brain volume loss respond to a potent IRT treatment strategy 11 years after diagnosis? This patient understands there is no data on natalizumab-switchers to support her request, but she is willing to take the risk of either alemtuzumab or HSCT. What do I advise her?
HELP! It is not easy being an MSologist. Please note these two scenarios are based on real patients of mine and are not hypothetical and represent the MS world I live and practice in.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
She is only 24 years of age; a graduate trainee in a marketing company. She has a promising future ahead of her. She lives in London and has a long term partner; they met at University. She knows he is the one for her and they are planning to get engaged in the next 1 to 2 years. Like most graduate trainees they find London expensive and share a house with four other people. She has found lockdown very stressful not because she has had to work from home with four other people, but because she was diagnosed with MS in February last year.
Despite starting DMF (Tecfidera) in June 2020, she had a very disabling relapse over the Christmas period with lower limb weakness and new-onset bladder symptoms. She has also noted a fine tremor in her right hand. Her latest MRI showed several new lesions and a large lesion in her thoracic spinal cord. Her consultant neurologist has offered her ocrelizumab. However, after doing her own online research including reading The MS-Blog (formerly known as the Barts-MS blog) she has asked to be treated with alemtuzumab. Her consultant has said no and pointed out their centre has virtually stopped using alemtuzumab because as a treatment it is too risky and there are much safer options.
Out of desperation this patient went to see a colleague of mine in private who said of course she can have alemtuzumab and she has now been referred to our centre for treatment. We are now in the process of doing the baseline bloods and will hopefully get this patient treated with her first course of alemtuzumab in the next few weeks. Tragically this poor woman has lost time. What would happen if in the interim she has a further catastrophic spinal cord relapse that leaves her paralysed? Who would be responsible?
I am beginning to refer to my colleagues who are not prepared to offer and use alemtuzumab and HSCT as the ‘refuseniks’. What they don’t realise is that they are putting themselves and their institutions at risk from legal challenge. How come? When NICE (National Institute of Health and Care Excellence) was created it was done so via an act of parliament. NICE’s primary aim was to get rid of the curse of postcode prescribing and variable access to treatments. Therefore if a therapy has been NICE approved the NHS has a legal obligation to offer people a specific treatment if they are eligible for that treatment. Therefore, in the case above her previous consultant is breaking the law and putting not only him or herself at risk of a legal challenge, but the relevant NHS Trust as well.
In 2021 why are neurologists still so paternalistic? Not allowing patients to choose their own treatment is against one of the central tenets of modern medicine. In reality, it is not the neurologist or the institution where the neurologist works who are taking a risk when someone is treated with alemtuzumab, it is the patient who is taking the risk. Don’t they understand this? It is getting to the point in time when we are going to have to start naming and shaming these refusenik neurologists. Hopefully, when the national audit figures from blueteq, NHS England’s database of high-cost drugs, is published those centres who are not prescribing alemtuzumab or offering referral for HSCT will be exposed. I am of the opinion that if you are not using alemtuzumab or HSCT in a proportion of your patients with highly active MS then you and your centre are not managing MS the way it should be managed in 2021.
I am sure not all of my neurology colleagues will agree with me; do you?
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
The ABN have updated their COVID-19 guidelines, which are beginning to move towards the evidence. However, the guidance on cladribine is not supported by the evidence nor the science, i.e. how cladribine actually works and its impacts the immune system.
The latest guidance states “the risk of severe COVID-10 disease is increased for many months after ocrelizumab and cladribine”. I am not sure there is evidence to support the statement about cladribine. Ocrelizumab and other anti-CD20 therapies are given continuously and hence the risk does not go away. However, cladribine is an immune reconstitution therapy and is reversible. Even in the depletion phase of treatment, the level of immunodepletion is modest, particularly for CD8+ T cells (see slide show below) and innate immunity is left intact. In our opinion, this pattern of immunodepletion is not sufficient to pose a risk to people with MS treated with cladribine and is supported by the emerging pharmacovigilance data.
The good news is that the guidelines state that for both ocrelizumab and cladribine “self-isolation for all that time is not appropriate except for individuals with multiple other risk factors”, which is compatible with our practice.
I am also reassured that their guidance has also softened for alemtuzumab; i.e. “we would anticipate pwMS being advised to strictly self-isolate for at least four weeks after an alemtuzumab administration”. This has been our practice since we started dosing alemtuzumab again. The rationale for the 4 week time period I assume is based on the impact of alemtuzumab on innate immunity and is supported by trial data; i.e. the viral infection risk falls rapidly after four weeks, presumably because monocyte counts recover.
The ABN is also recommending two weeks of self-isolation after high-dose steroids, which is pragmatic advice based on the risk of severe COVID-19 identified in the Italian registry studies.
The new guidance has also made a comment about vaccine readiness; “patients contemplating ocrelizumab should be advised that they may not be able to receive a future SARS CoV2 vaccine if it is a live vaccine, and they may not respond immunologically to a dead or inactivated vaccine. Consideration should be given to delaying ocrelizumab re-treatment”. It is interesting that none of the other DMTs is specifically mentioned when it comes to vaccine readiness. I am sure live viral vaccines will also be contraindicated in patients on S1P modulators (fingolimod and siponimod) and on some of the other immunosuppressive DMTs such as natalizumab and possibly even teriflunomide based on their current SmPCs.
The interesting thing about vaccine readiness is we don’t know about how important T-cell responses are in relation to these emerging vaccines and whether or not people on anti-CD20 therapies will mount an adequate protective T-cell response to the SARS-CoV-2 spike protein and other antigens. Everyone focuses on antibody responses when they may not be that important in protective anti-SARS-CoV-2 immunity.
I am sure we haven’t heard the last on MS DMTs and vaccine readiness. This is why I would urge all the DMT manufacturers to do the necessary studies to provide us with the necessary evidence-base to make clinical decisions.
I continue to be amazed when I hear senior MS neurologists make the claim they have never prescribed alemtuzumab or referred any of their patients for HSCT and don’t intend to do so either. These same neurologists seem to be happy with natalizumab and ocrelizumab as their #1 high-efficacy go to DMTs. When I challenge them with the exceptional longterm outcomes for pwMS treated early with alemtuzumab or HSCT I get a glazed look, which I now learnt is cognitive dissonance.
“Cognitive dissonance refers to a situation involving conflicting attitudes, beliefs or behaviours. This produces a feeling of mental discomfort leading to an alteration in one of the attitudes, beliefs or behaviours to reduce the discomfort and restore balance. For example, when people smoke (behaviour) and they know that smoking causes cancer (cognition), they are in a state of cognitive dissonance.” Source: Simply Psychology
It is quite clear that both ocrelizumab and natalizumab are very effective DMTs at switching-off focal inflammatory disease activity in MS; a large number of pwMS on these therapies are NEDA-2 (relapse-free and no new T2 lesions on MRI). This is interpreted by these neurologists and the wider MS community that MS is all sorted. Go away, get on with your life and be happy.
What these neurologists don’t tell their patients on ocrelizumab and natalizumab that despite no relapses or new MRI lesions the accelerated brain volume loss due to MS is continuing unabated. These neurologists and their patients are being lulled into a sense of false security because they believe MS is focal inflammatory disease, when in fact the real MS is the smouldering disease, which drives end-organ damage.
I have addressed these topics many times on this blog. If you are interested in reading some of my back catalogue of posts on this particular topic you can start with the posts below or you could watch a recent lecture I have given on the topic.
It is clear that not all DMTs are made equal when it comes to preventing end-organ damage. At the top of the league table are alemtuzumab and HSCT (~0.2-0.25% loss per annum). Both these treatments are NIRTs (non-selective immune reconstitution therapies).
Natalizumab is probably next with an annual brain volume loss in the region of 0.25-0.30% per annum. Ocrelizumab (anti-CD20) comes next with a rate of brain volume loss of ~0.374% per annum (see latest data below).
Why do natalizumab and ocrelizumab, despite being very effective anti-inflammatory DMTs have only a moderate impact on end-organ damage? This and other observations have convinced me that MS is not focal inflammation, which represents the immune system’s response to what is causing MS. I suspect there is something going in the CNS of pwMS that is the real MS; I refer to this hypothesis as the ‘Field Hypothesis’.
What these observations are telling us that peripheral B-cells are an important part of the immune response to the cause of MS, but B-cells are not necessarily involved in driving the true MS pathology, which is causing the progressive brain volume loss.
What does this mean for the well-informed person with MS? Firstly, you and your neurologist may not want to dismiss alemtuzumab and HSCT as a first-line, or at least early, treatment option. These non-selective highly effective IRTs differ from anti-CD20 therapies in that they target both B and T cells. I suspect we need to target both these cells types early in the course of the disease to really get on top of the real MS.
I am aware of the appeal of anti-CD20 therapies and natalizumab in that they are safer and easier to use because of less monitoring, however, this may come at a cost in the long-term. Please remember that once you have lost brain you can’t get it back. With alemtuzumab and HSCT, the risk is frontloaded, and balanced against the potential long-term gains in efficacy, which are unprecedented. Choosing a DMT on a rung or two lower down on the therapeutic ladder gives you better short-term safety and makes the life of your MS neurologist less stressful, because of less monitoring and fewer risks, but at a potential long-term cost to your brain and spinal cord.
This is why making an informed decision about which DMT you choose is a very complicated process and subject to subtle and often hidden effects of cognitive biases; cognitive dissonance is just one of these biases. The one bias I am very aware of is the ‘Gambler’s Dilemma’, be careful not to be lulled into a false sense of security by your beliefs; most gamblers eventually end-up losing.
In reality, we need to move treatment target in MS way beyond NEDA-2 to target end-organ damage, i.e. brain volume loss, T1 black holes, the slowly expanding lesions (SELs), neurofilament levels, cognition, sickness behaviour, OCBs, etc. Our treatment aim should be to ‘Maximise Brain Health’ across your life and not just the next few years.
As yet we don’t know what the impact of alemtuzumab and HSCT are on the pathology of smouldering MS, but these agents must be doing something to these pathologies based on clinical and MRI outcomes (see below). Despite this data gap, I think we have enough empirical evidence that alemtuzumab and HSCT are doing some fundamental to the pathology of MS.
Coming back to cognitive dissonance. It could be argued that if an MS neurologist or MS centre does not offer alemtuzumab or HSCT to at least some of their patients then they are not providing their patients with sufficient choice. In addition, they will almost certainly not accept the concept of smouldering MS being the real MS.
Objective: To assess over 3 years of follow-up, the effects of maintaining or switching to ocrelizumab (OCR) therapy on clinical and MRI outcomes and safety measures in the open-label extension (OLE) phase of the pooled OPERA studies in relapsing multiple sclerosis.
Methods: After 2 years of double-blind, controlled treatment, patients continued OCR (600 mg infusions every 24 weeks) or switched from interferon (IFN) β-1a (44 μg 3 times weekly) to OCR when entering the OLE phase (3 years). Adjusted annualized relapse rate, time to onset of 24-week confirmed disability progression/improvement (CDP/CDI), brain MRI activity (gadolinium-enhanced and new/enlarging T2 lesions), and percentage brain volume change were analyzed.
Results: Of patients entering the OLE phase, 88.6% completed Year 5. The cumulative proportion with 24-week CDP was lower in patients who initiated OCR earlier, vs patients initially receiving IFN β-1a (16.1% vs 21.3% at Year 5; p=0.014). Patients continuing OCR maintained, and those switching from IFN β-1a to OCR attained near complete and sustained suppression of new brain MRI lesion activity from Year 3 to 5. Over the OLE phase, patients continuing OCR exhibited less whole brain volume loss from double-blind study baseline vs those switching from IFN β-1a (–1.87% vs –2.15% at Year 5; p<0.01). Adverse events were consistent with past reports and no new safety signals emerged with prolonged treatment.
Conclusion: Compared with patients switching from IFN β-1a, earlier and continuous OCR treatment up to 5 years provided sustained benefit on clinical and MRI measures of disease progression.
Classification of evidence: This study provides Class III evidence that earlier and continuous treatment with ocrelizumab provided sustained benefit on clinical and MRI outcomes of disease activity and progression compared with patients switching from IFN β-1a. The study is rated Class III because of the initial treatment randomization disclosure that occurred after inclusion in OLE.
BACKGROUND: A cohort of patients with poor-prognosis multiple sclerosis (MS) underwent chemotherapy-based immune ablation followed by immune reconstitution with an autologous hematopoietic stem cell transplant (IA/aHSCT). This eliminated new focal inflammatory activity, but resulted in early acceleration of brain atrophy.
OBJECTIVE: We modeled the time course of whole-brain volume in 19 patients to identify the baseline predictors of atrophy and to estimate the average rate of atrophy after IA/aHSCT.
METHODS: Percentage whole-brain volume changes were calculated between the baseline and follow-up magnetic resonance imaging (MRI; mean duration: 5 years). A mixed-effects model was applied using two predictors: total busulfan dose and baseline volume of T1-weighted white-matter lesions.
RESULTS: Treatment was followed by accelerated whole-brain volume loss averaging 3.3%. Both the busulfan dose and the baseline lesion volume were significant predictors. The atrophy slowed progressively over approximately 2.5 years. There was no evidence that resolution of edema contributed to volume loss. The mean rate of long-term atrophy was -0.23% per year, consistent with the rate expected from normal aging.
CONCLUSION: Following IA/aHSCT, MS patients showed accelerated whole-brain atrophy that was likely associated with treatment-related toxicity and degeneration of “committed” tissues. Atrophy eventually slowed to that expected from normal aging, suggesting that stopping inflammatory activity in MS can reduce secondary degeneration and atrophy.
OBJECTIVE: To describe detailed MRI results from 2 head-to-head phase III trials, Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis Study I (CARE-MS I; NCT00530348) and Study II (CARE-MS II; NCT00548405), of alemtuzumab vs subcutaneous interferon β-1a (SC IFN-β-1a) in patients with active relapsing-remitting multiple sclerosis (RRMS).
METHODS: The impact of alemtuzumab 12 mg vs SC IFN-β-1a 44 μg on MRI measures was evaluated in patients with RRMS who were treatment-naive (CARE-MS I) or who had an inadequate response, defined as at least one relapse, to prior therapy (CARE-MS II).
RESULTS: Both treatments prevented T2-hyperintense lesion volume increases from baseline. Alemtuzumab was more effective than SC IFN-β-1a on most lesion-based endpoints in both studies (p < 0.05), including decreased risk of new/enlarging T2 lesions over 2 years and gadolinium-enhancing lesions at year 2. Reduced risk of new T1 lesions (p < 0.0001) and gadolinium-enhancing lesion conversion to T1-hypointense black holes (p = 0.0078) were observed with alemtuzumab vs SC IFN-β-1a in CARE-MS II. Alemtuzumab slowed brain volume loss over 2 years in CARE-MS I (p < 0.0001) and II (p = 0.012) vs SC IFN-β-1a.
CONCLUSIONS: Alemtuzumab demonstrated greater efficacy than SC IFN-β-1a on MRI endpoints in active RRMS. The superiority of alemtuzumab was more prominent during the second year of both studies. These findings complement the superior clinical efficacy of alemtuzumab over SC IFN-β-1a in RRMS.
CLASSIFICATION OF EVIDENCE: The results reported here provide Class I evidence that, for patients with active RRMS, alemtuzumab is superior to SC IFN-β-1a on multiple MRI endpoints.
BACKGROUND: Tissue damage in both multiple sclerosis (MS) lesions and normal-appearing white matter (NAWM) are important contributors to disability and progression. Specific aspects of MS pathology can be measured using advanced imaging. Alemtuzumab is a humanised monoclonal antibody targeting CD52 developed for MS treatment.
OBJECTIVE: To investigate changes over 2 years of advanced magnetic resonance (MR) metrics in lesions and NAWM of MS patients treated with alemtuzumab.
METHODS: A total of 42 relapsing-remitting alemtuzumab-treated MS subjects were scanned for 2 years at 3 T. T1 relaxation, T2relaxation, diffusion tensor, MR spectroscopy and volumetric sequences were performed. Mean T1 and myelin water fraction (MWF) were determined for stable lesions, new lesions and NAWM. Fractional anisotropy was calculated for the corpus callosum (CC) and N-acetylaspartate (NAA) concentration was determined from a large NAWM voxel. Brain parenchymal fraction (BPF), cortical thickness and CC area were also calculated.
RESULTS: No change in any MR measurement was found in lesions or NAWM over 24 months. BPF, cortical thickness and CC area all showed decreases in the first year followed by stability in the second year.
CONCLUSION: Advanced MR biomarkers of myelin (MWF) and neuron/axons (NAA) show no change in NAWM over 24 months in alemtuzumab-treated MS participants.
This week I am doing video consultations with all the volunteers who participated in the pivotal phase 3 and 10-year extension studies of the alemtuzumab clinical trials. My objectives are three-fold. Firstly, to make sure they are referred back into a routine NHS MS service and are not left floundering without follow-up. Secondly, to complete a few exit EDSS examinations of the last few subjects and thirdly, and most importantly, to thank them for their time and commitment to these trials.
During my video consultations, it dawned on me that I have never seen a cohort of patients doing so well 10+ years into their MS disease course. The majority are NEDA (no disease activity) fully functional and participating fully in life. Yes, fully in life; married, in civil and other partnerships, working, with families, playing sports, participating in creative activities, volunteering and with very few symptomatic MS problems. Yes, a few of them have thyroid problems, but these are all being managed without a major impact on these patients lives.
I am convinced that some of these trial subjects may actually be cured of having MS. I am witnessing something extraordinary and at the same time something very sad. Why have we, the MS community, not adopted early alemtuzumab treatment as the standard of care? Why wouldn’t you want to take a chance on a treatment that maximises your chances of staying fully functional and may even offer a cure?
The patients who are not doing so well, unfortunately, got onto alemtuzumab late and therein lies the epiphany; early highly-effective treatment is the only way to realistically slay this beast. Knowing what I know, if I had MS I would have no hesitation being treated with alemtuzumab or even HSCT.
The tragedy is that the MS community and the regulators have killed alemtuzumab relegating it to a second or in most countries a third or fourth line agent. This is an international tragedy and I am not sure if we will ever get alemtuzumab back to its rightful place as a first-line treatment option for early active MS.
Alastair Compston, his protege Alasdair Coles and the Cambridge team deserve all the plaudits for getting this innovation to the clinic. However, sometimes this is just not enough to get wide adoption of an extraordinary innovation.