Barts-MS rose-tinted-odometer: ★★★ (I am seeing blue and Spanish yellow today) Roche blue (#0066CC) & Novartis Spanish Yellow (#F7B516)
Yes, I really do think that intrathecal (within the meninges that cover the brain and spinal cord) or CNS resident B-cells and plasma cells are pathogenic in MS. In other words, the cytokine or chemicals B-cells and plasma cells produce, in particular their antibodies, are what is driving some of the pathologies of smouldering MS. The evidence to support this hypothesis is well rehearsed on this blog and is the reason why we are testing high-dose ocrelizumab (more CNS penetrant) vs. standard-dose ocrelizumab (less CNS penetrant) against each other in two head-2-head studies. It is also the reason we are testing cladribine’s (CLADRIPLAS and CLAD-B) and ixazomib’s (SIZOMUS) effects in intrathecal B and plasma cell markers. Yes, I really do think we need to scrub the CNS clean of B-cells, plasma cells and their products, in particular the oligoclonal IgG bands.
I am therefore proposing a new study; the HIgh-dose versus LOw-dose anti-CD20 study or HILO Study.
In this study, I propose testing high-dose or double-dose ocrelizumab vs. standard or intermediate-dose ocrelizumab vs. low-dose ofatumumab against each other over two years and measure their impact on end-organ damage markers (slowly expanding lesions and brain volume loss) and on CSF markers of B-cell, plasma cell and microglial activity. The latter will include free kappa and lambda immunoglobulin light chains, OCBs, soluble CD14, etc. This will answer at least from a biomarker question whether or not we need CNS penetration of anti-CD20 monoclonal antibodies to target this component of smouldering MS. The following would also answer the question of whether or not you as a person with MS would want to be treated with high-dose or low-dose anti-CD20 therapy?
Would you want to be randomised into this study?
This study would be a clash of the titans; Roche vs. Novartis. Who would win? It really is not that important as Novartis is a major shareholder in Roche and hence when Roche makes a profit so does Novartis. The real winners will be people with MS, the data will allow them to make an informed decision about whether or not they want to go beyond NEIDA (no evident inflammatory disease activity) and be on a treatment that tackles the smouldering B-cell and plasma-cell driven processes within their brains and spinal cords.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.
Barts-MS rose-tinted-odometer: ★★★ (It feels like a sky blue rainy Friday = #87ceeb)
“Prof G how many of my monthly ofatumumab injections should I miss to guarantee that I will have an adequate antibody response to the COVID-19 vaccine?”
This was the gist of one of the direct messages I received on Twitter from a person with MS living in the US.
I really don’t know. However, I have tried extrapolating data from the repopulation kinetics of ofatumumab given 3-monthly and the modelling data below on ocrelizumab and rituximab. For ocrelizumab and rituximab to have 80% confidence it requires at least 9 months from the last infusion to the first vaccination to have a >50% chance of seroconversion in response to an RNA-based COVID-19 vaccine. This equates to missing close to one dose of ocrelizumab or rituximab as you have to wait 9 months then have two vaccine doses and wait 3-4 weeks after your second or booster dose of vaccine before recommencing your 6-monthly infusions. i.e. ~11 months after your last infusion. Although Mike Famulare has treated rituximab and ocrelizumab as being equipotent in his modelling I suspect he is wrong and the gap for ocrelizumab may in fact have to be substantially longer. I predict that the average person will need to wait about 11-12 months post their last infusion of ocrelizumab to be confident of an antibody response.
As ofatumumab, is a lower dose anti-CD20, with more rapid B-cell repopulation kinetics than ocrelizumab or rituximab (see figure below). I estimate that you will need to wait about 6 months from your last injection before being vaccinated and you would then have two vaccine doses and wait 3-4 weeks after your second or booster dose of vaccine before recommending your monthly injections. i.e. ~8 months later. As this is all based on modelling I suspect in real life you will simply need to wait for peripheral blood B-cell reconstitution to occur before being vaccinated. The problem with the latter is how high do your peripheral B-cells have to be before being vaccinated; more than 3, 5, 10, 20, 50 or 80 CD19+ B-cells per mm3? Clearly, this is something that needs further study and I would urge Pharma or one of the MS groups interested in answering this question to do the study. Let’s call it the ‘Peripheral B-cell Threshold Vaccine Study‘ or the ‘PerBeC Vax Study‘.
I want to reiterate that vaccine immunity is not only about B-cell and antibody immunity, T-cells also have an important role to play. Granted that if you don’t make antibodies it indicates that your follicular T-helper cells memory may not be that great, but this does not tell you about other CD4+ and CD8+ T-cell memory responses. Therefore, please be patient until these data emerge.
My message remains the same; #GetVaccinatedASAP. During this phase of the pandemic, some immunity is better than no immunity. The risk associated with getting COVID-19, particularly if you are on a B-cell depleting agent, far outweighs the risks associated with vaccination.
Seroconversion rate following complete COVID-19 vaccination vs. time since most recent b-cell depleting therapy (BCDT). Best fit, 80%, and 95% confidence interval shows logistic regresssion model of seroconversion probability over time.
B-cell depleting therapies (BCDT) such as ocrelizumab and rituximab used for the management of multiple sclerosis are associated with reduced seroconversion rates following COVID-19 vaccination. In this note, I reanalyze data from the literature to examine how the probability of seroconversion depends on the time interval between the last BCDT dose and the first vaccine dose. While uncertainty is high due to limited data, the results show that the seroconversion probability increases with time. Under a Bayesian interpretation of logistic regression, I estimate with 80% confidence that it requires at least 9 months from last BCDT to first vaccination to have a >50% chance of seroconversion following complete mRNA vaccination, with large uncertainty on when higher confidence of seroconversion can be expected. Among subjects who do seroconvert following vaccination, anti-Spike IgG levels correlate with time since last BCDT. Limited data indicate that levels comparable with immunocompetent response can be achieved with intervals of 12 or more months between BCDT and vaccination. With combined data from multiple sources, I argue that time development of the seroconversion probability and antibody response parallels that of CD19+ and naive B-cell repopulation following BCDT, suggesting that monitoring B-cell repopulation will be useful at the individual level for optimizing vaccine response while maintaining adequate MS control.
Pharmacodynamic response showing dose-response depletion of CD19 B cells and repletion kinetics (safety population). The median time to repletion based on Kaplan-Meier estimates was ≈11 months for the ofatumumab 3 and 30 mg every 12 weeks groups and ≈14 months for the ofatumumab 60 mg every 12 and 4 weeks groups.
Objective: To assess dose-response effects of the anti-CD20 monoclonal antibody ofatumumab on efficacy and safety outcomes in a phase 2b double-blind study of relapsing forms of multiple sclerosis (RMS).
Methods: Patients (n = 232) were randomized to ofatumumab 3, 30, or 60 mg every 12 weeks, ofatumumab 60 mg every 4 weeks, or placebo for a 24-week treatment period, with a primary endpoint of cumulative number of new gadolinium-enhancing lesions (per brain MRI) at week 12. Relapses and safety/tolerability were assessed, and CD19+ peripheral blood B-lymphocyte counts measured. Safety monitoring continued weeks 24 to 48 with subsequent individualized follow-up evaluating B-cell repletion.
Results: The cumulative number of new lesions was reduced by 65% for all ofatumumab dose groups vs placebo (p < 0.001). Post hoc analysis (excluding weeks 1-4) estimated a ≥90% lesion reduction vs placebo (week 12) for all cumulative ofatumumab doses ≥30 mg/12 wk. Dose-dependent CD19 B-cell depletion was observed. Notably, complete depletion was not necessary for a robust treatment effect. The most common adverse event was injection-related reactions (52% ofatumumab, 15% placebo), mild to moderate severity in 97%, most commonly associated with the first dose and diminishing on subsequent dosing.
Conclusion: Imaging showed that all subcutaneous ofatumumab doses demonstrated efficacy (most robust: cumulative doses ≥30 mg/12 wk), with a safety profile consistent with existing ofatumumab data. This treatment effect also occurred with dosage regimens that only partially depleted circulating B cells.
Classification of evidence: This study provides Class I evidence that for patients with RMS, ofatumumab decreases the number of new MRI gadolinium-enhancing lesions 12 weeks after treatment initiation.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
Barts-MS rose-tinted-odometer: ★★ (amber; a sleep deprived colour somewhere between yellow and orange)
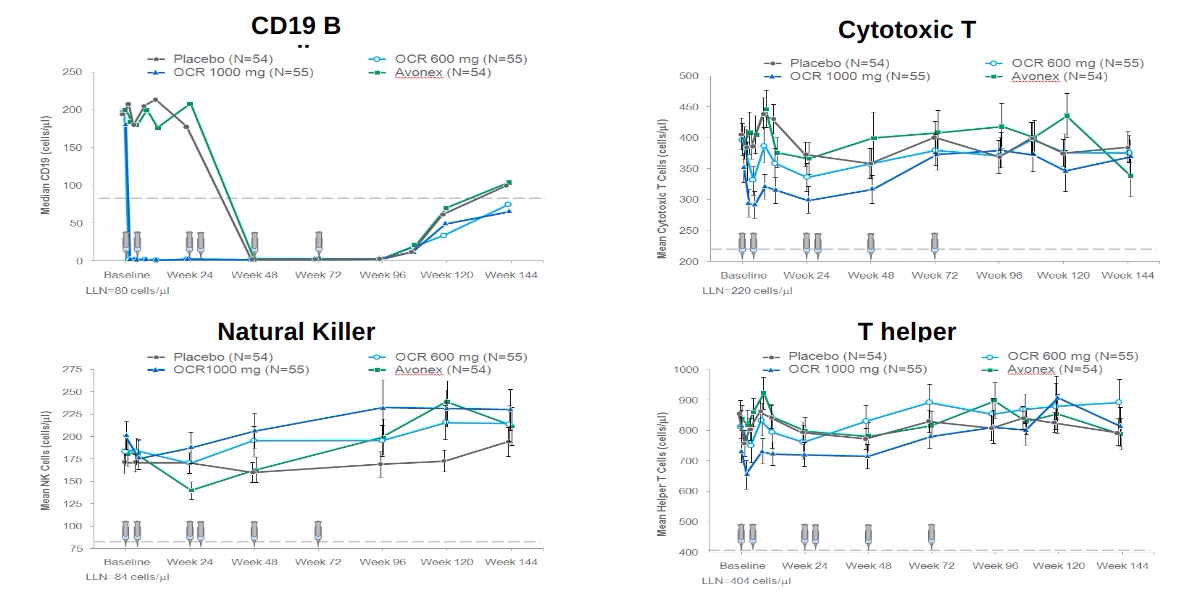
It has become clear that the anti-CD20 therapies are more than just anti-B-cell therapies. Minority populations of both CD4+ and CD8+ T-cells and NK-cells express CD20 and are depleted after both rituximab and ocrelizumab treatment.
It looks as if ocrelizumab may be more effective in deleting this population of cells and may explain why herpes zoster or shingles is more common after ocrelizumab, compared to rituximab, than what you would expect based on its putative B-cell only targeting effect. The mild depletion of this population of cells may also explain why pwMS on ocrelizumab are at higher risk of getting COVID-19 and severe COVID-19.
The study below shows that this population of cells express a so-called CTL or cytotoxic phenotype that fits in with the zoster and COVID-19 data. This also raises concerns that just maybe peripheral tumour immune surveillance is also compromised on anti-CD20 therapies. The tumour signal however is likely to be small as a large secondary cancer signal would likely have emerged already on the anti-CD20s.
More topical is the role these CD20-expressing T-cells play in vaccine responses. If they are important in vaccine immunity then patients with MS on anti-CD20 therapies who lack this population of T-cells may not develop adequate T-cell immunity in response to vaccination. We won’t have long to wait for the latter data as many immunology laboratories are busy trying to get their T-cell vaccine data out as soon as possible.
So yes there is much more to the immunology of anti-CD20 therapy than simple B-cell depletion. Could the T-cell compartment targeted by anti-Cd20 therapies be as important or more important than the B-cell compartment? There is so much more to learn about how MS DMTs really work, in particular the anti-CD20 therapies.
Recently, it was shown that highly effective anti-CD20 therapies used for MS patients not only deplete CD20+ B cells, but also a small subset of T cells expressing CD20 surface marker (CD3+CD20+ T cells). Here we demonstrated that, in progressive MS patients, CD3+CD20+ T cells share the ability to express cytotoxic factors such as perforin and serine-protease granzyme-B (GzmB), classically associated with CD8+ T cells functionality. Beyond it, cluster analyses show that a set of activation markers and transcriptional factors related with CD8 effector program are also expressed in CD3+CD20+ T cells. Further characterization of surface and functional markers from CD3+CD20+ T subsets may be helpful for development of new therapeutic strategies mainly for progressive MS patients, as well as for assessing pathophysiological effects of highly effective anti-CD20 therapies.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
As you know the vast majority of pwMS on anti-CD20 therapy who get COVID-19 or for that matter any other viral infection recover. In other words, their immune systems work despite blunted or absent B-cell or antibody responses. This study presented yesterday at the AAN meeting confirms that ocrelizumab-treated patients who get COVID-19 have good robust T-cell responses. Almost all of these patients also had antibody responses to the virus. The ocrelizumab-treated cases that fail to seroconvert may therefore represent a publication bias. However, as this study doesn’t include the 5% of subjects on ocrelizumab who succumb to COVID-19 we can’t assume this applies to all ocrelizumabers.
It will be interesting to see these results replicated with the COVID-19 vaccines. Although wild-type infection with SARS-CoV-2 is likely to provide a more robust immunological challenge than a COVID-19 vaccine, I can’t see why the vaccine won’t induce T-cell responses as well. The question will be how few patients fail to respond to the vaccine at both an antibody and T-cell level.
I am sure a large number of ocrelizumabers or anti-CD20ers and their HCPs will be relieved to see these results (or not).
Objective: 1. To assess SARS-CoV-2 seropositivity in 1,000 patients with multiple sclerosis (MS) and its association with demographic and disease-related characteristics, and disease-modifying therapy (DMT); 2. To evaluate the persistence of antibody and T-cell responses in a subset of these patients who were receiving ocrelizumab (OCR), other DMT or no DMT at the time of COVID-19 infection. Background: Since March 2020, ˜15% of patients attending NYU MS Care Center (NYUMSCC) in New York City had COVID-19. It is unknown whether DMTs affect the persistence of antibody and T-cell responses to SARS-CoV-2.
Design/Methods: Patients from NYUMSCC were invited to undergo serologic assessment using Elecsys Anti-SARS-CoV-2 (Roche Diagnostics) and multiplex bead-based immunoassays of antibody responses to SARS-CoV-2 nucleocapsid and spike proteins. A subset of patients with or without COVID-19 history underwent a study of T-cell responses to SARS-CoV-2 spike protein using IFN-? enzyme-linked immunosorbent spot (Invitrogen) and TruCulture (Myriad RBM) spike protein assays and live virus immunofluorescence-based microneutralization assay.
Results: Since January 2021, 100 unvaccinated patients with MS were enrolled (mean 41 years; 63% female; 45% non-white; 35% on OCR; 26% had COVID-19). Antibody and T-cell results were available for 40 patients (26 on OCR; 17 had COVID-19, median 10 months before sampling). Of the 40, Elecsys Anti- SARS-CoV-2 assay identified all but 2 COVID-19+ patients, and multiplex bead-based assay identified all but 1 COVID-19+ patient as seropositive. Neither assay had false positives. T-cell activation based on induced IFN-gamma secretion was observed in 10/17 COVID-19+ patients and 1 patient without COVID-19 history who developed PCR-confirmed COVID-19 five days after sampling. Anti-SARS-CoV-2 antibody response was detected in 4/5 and T-cell response in 3/5 OCR-treated COVID-19+ patients.
Conclusions: Preliminary results suggest persistent humoral and T-cell immune memory to SARS-CoV-2 up to 10 months following infection even in B-cell depleted patients with MS. Updated results will be presented.
Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the position of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.