Barts-MS rose-tinted-odometer: ★ (Bank Holiday Monday morning blues)


The next marketing battle in terms of MS DMTs will be herpes zoster and how we manage it. Shingles is quite common in the general population, but it is much more common in pwMS. Why? Probably because of the immunosuppression associated with MS DMTs and the use of high-dose steroids to treat relapses and prevent infusion reactions. Put simply Zoster comes with the territory of managing MS. The following figure is from a meta-analysis I have recently done on the rate of zoster reactivation on current MS DMTs relative to other DMTs and compared to what is expected in the background population. Do you find the results surprising?


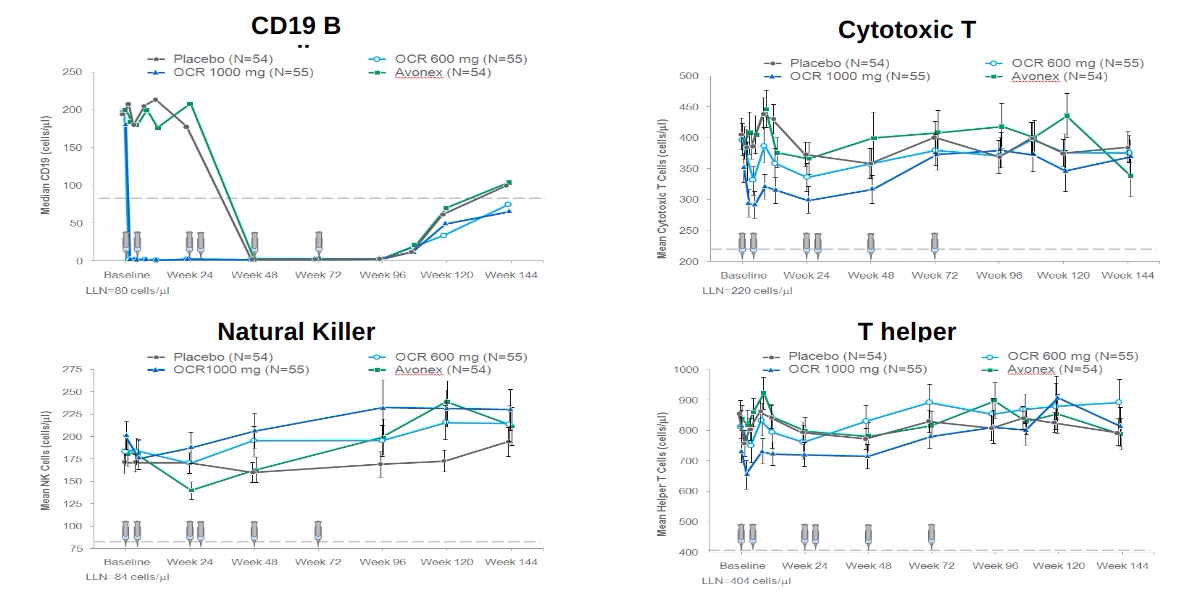
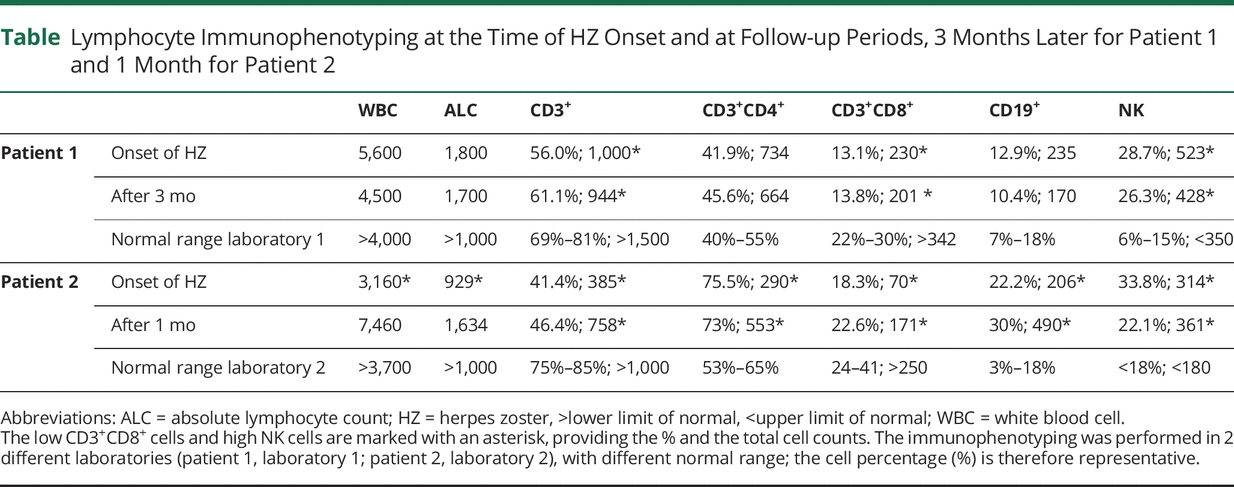
The two reported case studies below of severe shingles/herpes-zoster in two pwMS on dimethyl fumarate demonstrates two things. Firstly, contrary to what most people think DMF is an immunosuppressive compound. Even if we derisk DMF and switch treatments if the total lymphocyte counts drop below 880/mm3 or 500/mm3 there can still be quite a profound CD8+ T-cell lymphopaenia. Secondly, the cases below actually had relatively normal total lymphocyte counts despite low CD8+ T-cell counts. These cases make me wonder if we should be monitoring T-cells subset counts in our patients on DMF.
The relative sensitivity of CD8+ T-cells to DMF must be a clue to how the drug is working from an immunological perspective. Despite this, the exact mode of action of DMF in MS remains a mystery.
For several years I have been asking whether or not boosting cytotoxic CD8+ T-cell immunity against the herpes zoster virus with the new Shringex vaccine, prior to starting DMTs, would lower the risk of shingles on treatment. Which brave Pharma company will do this study in the current environment? I suspect a few might take the plunge as vaccine readiness or vaccine responsiveness is now uppermost in the minds of MS experts and their patients. The latter is being driven by the COVID-19 vaccine studies and the demonstration that people on antiCD20 therapies and fingolimod of blunted antibody responses to the vaccines.
So in summary vaccines, vaccine readiness and derisking infectious complications, in particular herpes zoster, will be the next marketing battleground in the MS DMT wars. Did your HCP discuss the zoster risk with you prior to start you on a DMT?
Anagnostouli et al. Aggressive Herpes Zoster in Young Patients With Multiple Sclerosis Under Dimethyl Fumarate: Significance of CD8 + and Natural Killer Cells. Neurol Neuroimmunol Neuroinflamm. 2021 May 28;8(4):e1017.

General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.