The next marketing battle in terms of MS DMTs will be herpes zoster and how we manage it. Shingles is quite common in the general population, but it is much more common in pwMS. Why? Probably because of the immunosuppression associated with MS DMTs and the use of high-dose steroids to treat relapses and prevent infusion reactions. Put simply Zoster comes with the territory of managing MS. The following figure is from a meta-analysis I have recently done on the rate of zoster reactivation on current MS DMTs relative to other DMTs and compared to what is expected in the background population. Do you find the results surprising?
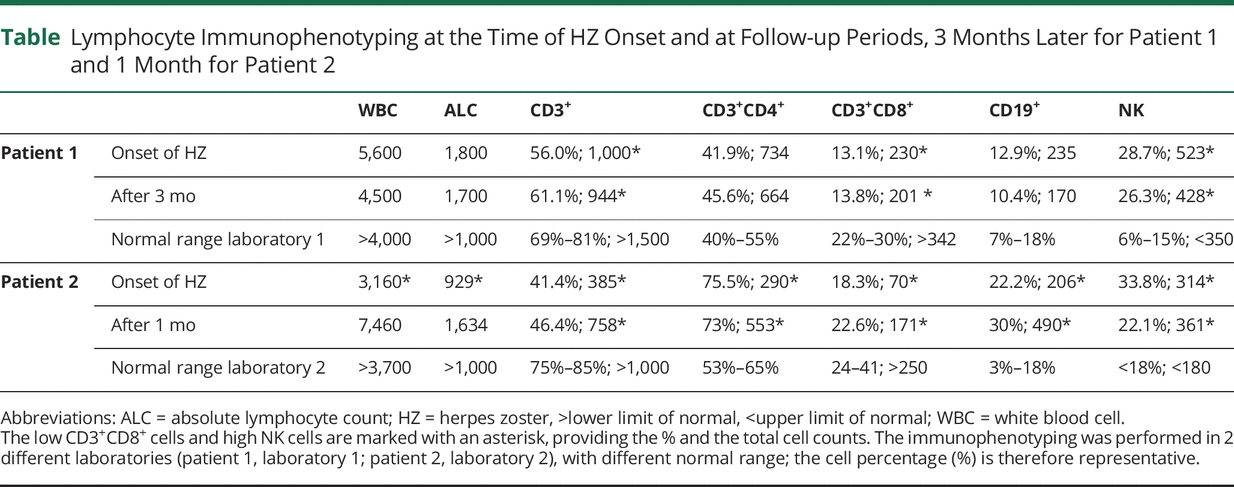
The two reported case studies below of severe shingles/herpes-zoster in two pwMS on dimethyl fumarate demonstrates two things. Firstly, contrary to what most people think DMF is an immunosuppressive compound. Even if we derisk DMF and switch treatments if the total lymphocyte counts drop below 880/mm3 or 500/mm3 there can still be quite a profound CD8+ T-cell lymphopaenia. Secondly, the cases below actually had relatively normal total lymphocyte counts despite low CD8+ T-cell counts. These cases make me wonder if we should be monitoring T-cells subset counts in our patients on DMF.
The relative sensitivity of CD8+ T-cells to DMF must be a clue to how the drug is working from an immunological perspective. Despite this, the exact mode of action of DMF in MS remains a mystery.
For several years I have been asking whether or not boosting cytotoxic CD8+ T-cell immunity against the herpes zoster virus with the new Shringex vaccine, prior to starting DMTs, would lower the risk of shingles on treatment. Which brave Pharma company will do this study in the current environment? I suspect a few might take the plunge as vaccine readiness or vaccine responsiveness is now uppermost in the minds of MS experts and their patients. The latter is being driven by the COVID-19 vaccine studies and the demonstration that people on antiCD20 therapies and fingolimod of blunted antibody responses to the vaccines.
So in summary vaccines, vaccine readiness and derisking infectious complications, in particular herpes zoster, will be the next marketing battleground in the MS DMT wars. Did your HCP discuss the zoster risk with you prior to start you on a DMT?
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.
During the COVID-19 pandemic, disease-modifying therapies (DMTs) have been scrutinised based on their mode of action and ability to cause immunosuppression. In general dimethyl fumarate has gotten off very lightly with most commentators referring it as an immunomodulator and being a relatively low-risk DMT should someone get COVID-19 on DMF. The latter is based on the assumption that DMF does not cause immunosuppression. I disagree with the latter assessment, but we need data. Where is the data?
How well are patients on DMF who get COVID-19 doing? I am aware that there are a lot of DMF-treated patients who have had COVID-19, but the investigators who have this information are being very slow at releasing their data. In fact, they have deliberately chosen to publish their data in high-impact journals rather than releasing it early into one of the prepublication archives. One could interpret this as them prioritising their academic ambitions above the concerns of the wider MS community during this crisis. The delay in getting this information to you is likely to be measured in months rather than weeks and is causing you anxiety. I personally think this is unacceptable.
In summary, DMF is an immunosuppressive therapy based on the five tests I apply when considering whether or not a drug is immunosuppressive.
1. Mode of action: DMF inhibits NF-κB (nuclear factor kappa B), which is one of the master transcription factors in controlling inflammation. You can’t be an NF-κB inhibitor and not be immunosuppressive.
2. Lymphopaenia: drugs that cause significant lymphopaenia tend to be immunosuppressive. Total lymphocyte counts drop on average by about 30% on DMF and about 15% of subjects lower their lymphocyte counts below 800/mm3 and 5% below 500/mm3. In addition, DMF has a greater impact on CD8+cells more than CD4+ cells, which may explain why there is a relatively large herpes zoster signal in DMF-treated patients. The following is the section on Zoster from the Tecfidera SmPC.
“Herpes zoster infections have been reported with Tecfidera use. In an ongoing long-term extension study, in which 1736 MS patients are treated with Tecfidera, approximately 5% experienced one or more events of herpes zoster, the majority of which were mild to moderate in severity. Most subjects, including those who experienced a serious herpes zoster infection, had lymphocyte counts above the lower limit of normal. Grade 2 and 3 lymphopenia prevailed in subjects with concurrent lymphocytopenia. In the post-marketing setting, most cases of herpes zoster infection were non-serious and resolved with treatment. Limited data is available on ALC in patients with herpes zoster infection in the post-marketing setting. However, when reported, most patients experienced grade 2 (< 0.8 × 109/L to 0.5 × 109/L) or grade 3 (<0.5 × 109/L to 0.2 × 109/L) lymphopenia (see section 4.4).”
3. Opportunistic infections: it is clear that there is a small opportunistic infection signal with DMF. It started with a few caes of PML and there has been a steady number of case reports of DMF-treated patients with different opportunistic infections. The case below of a patient presenting with cryptococcal meningitis an opportunistic fungal infection is an example. So if you are on DMF don’t think you are necessarily safe from infections you still need to be vigilant.
4. Vaccine responses: Vaccine responses to recall antigens (tetanus) and new antigens (meningococcus) were reasonable in DMF treated patients, but the response to the pneumococcal vaccine was variable. Differences in the response to both tetanus toxoid and pneumococcal serotype 3 polysaccharide antigen were less in MS patients on DMF compared to those on beta-interferon. Importantly there is no data on the effectiveness and safety of live vaccines in patients taking DMF. The SmPC in fact warns against live vaccines.
“Live vaccines might carry an increased risk of clinical infection and should not be given to patients treated with Tecfidera unless, in exceptional cases, this potential risk is considered to be outweighed by the risk to the individual of not vaccinating.”
Not being able to have live vaccines may be an issue for a SARS-CoV-2 as many of the candidate vaccines are using live viral vectors to deliver the immunogen.
5. Secondary malignancies: At present, there is no clear secondary malignancy signal on DMF. However, based on its mode of action and level of immunosuppression (relatively mild on average) a signal may take decades to emerge (known-unknown). An analogy is azathioprine monotherapy, a mild first-line immunosuppressive therapy, in which the secondary cancer risk (lymphoma) only emerges after 10 years of treatment. So again be vigilant particularly for skin cancers (squamous and basal cell carcinomas) and haematological malignancies which tend to be the sentinel cancers with longterm immunosuppression.
So in summary, the advice that DMF is safe if you get COVID-19 remains an opinion when the evidence is hidden behind several publication embargos. It is not an ideal DMT to be on if a live virus SARS-CoV-2 vaccine gets to market.
Introduction: We present a case of meningitis caused by Cryptococcus neoformans var. grubii in a 46-year old non-HIV-infected patient with multiple sclerosis, treated with dimethyl fumarate monotherapy. We identified no other risk factors for developing cryptococcal meningitis. The patient presented with a slowly progressive headache during preceding weeks and acute onset of confusion, nausea and vomiting. Clinical examination revealed intermittent disorientation without focal neurological symptoms. A lumbar puncture showed an opening pressure of > 50cmH2O. Diagnosis of cryptococcal meningitis was made after culture of Cryptococcus neoformans var. grubii of cerebrospinal fluid.
Conclusion: This case emphasizes clinicians should bear in mind the possibility of cryptococcal meningitis in patients treated with dimethyl fumarate.