Barts-MS rose-tinted-odometer: zero-★s (purple Sunday)


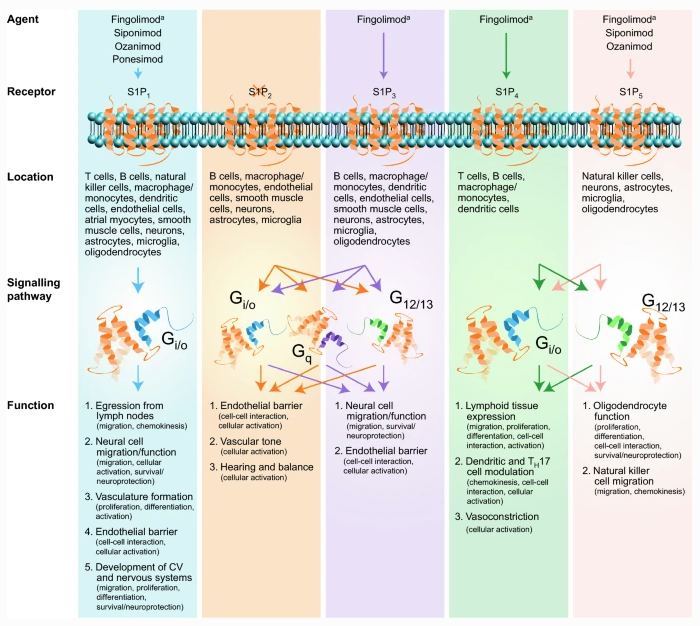
The following case suggests a horizontal switch from fingolimod to siponimod may not be the wisest thing to do. This patient developed severe fingolimod rebound despite switching to siponimod without a washout. As you know fingolimod works on 4 out of 5 of S1P receptors (S1P1, 3, 4, and 5). In comparison, siponimod works on S1P1 and S1P5 only. Is this telling us that some of the modes of action of the S1P modulators are via S1P3 and S1P4? I suspect Yes. S1P4 may be important for antigen presentation and germinal centre (GC) function in lymph nodes and other secondary lymphoid organs, which explains why COVID-19 vaccine responses are so flat in pwMS on fingolimod. If this is correct then we may see better vaccine response in patients on the other S1P modulators that don’t impact GC biology to the same extent.

I predict that there will be many more patients like this. The important thing is to ask why and to explore exactly what the differences are between fingolimod and siponimod on immune function in MS. Who knows what it is telling us about the cause and immunology of MS.


Published online 2021 May 15. doi: 10.1016/j.ensci.2021.100346
Senzaki et al. Disease reactivation in a patient with secondary progressive multiple sclerosis after switching treatment from fingolimod to siponimod. eNeurologicalSci. 2021 May 15;23:100346. doi: 10.1016/j.ensci.2021.100346.
Excerpt: …… A 42-year-old woman with RRMS was started on fingolimod due to high disease activity; three relapses in the previous year and the presence of gadolinium-enhancing brain lesions before fingolimod. During the first two years after initiation of fingolimod, she experienced several relapses with incomplete recovery and progressive increase in brain magnetic resonance imaging (MRI) lesion load, and her EDSS deteriorated from 3.5 to 5.5. In the next five years, she was relapse-free without MRI activity; however, her disability gradually worsened to EDSS score of 7.0 and she was diagnosed with SPMS. Fingolimod was switched to siponimod without a wash-out period. Peripheral lymphocyte count at initiation of siponimod (day 1) was 376/μL, and 433/μL at day 7. She developed double vision at day 11. Neurological examination revealed no new additional findings except for right internuclear ophthalmoplegia. Brain MRI showed multiple hyperintense infra- and supra-tentorial lesions on fluid-attenuated inversion-recovery images, some of which were enhanced with gadolinium (Fig. 1).
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust.