Barts-MS rose-tinted-odometer: ★★★ (a dark blue Saturday; a chastised weekend warrior #00008b )

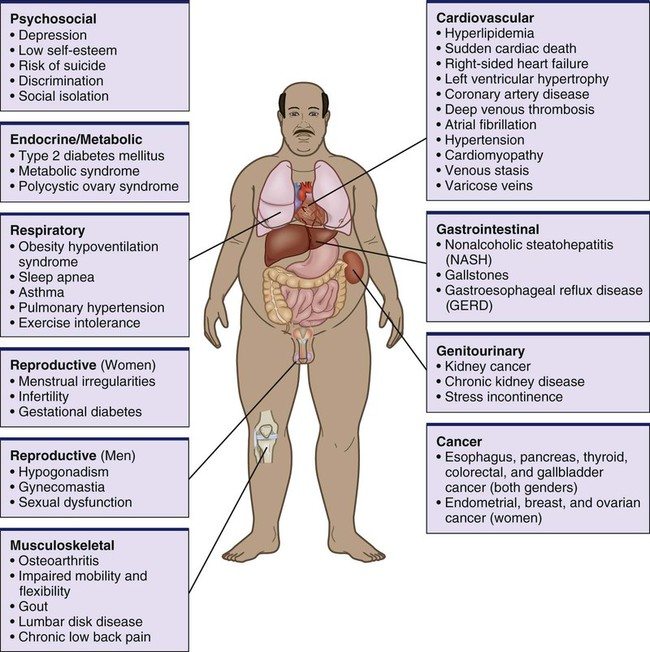
I was accused this week by some commentators on social media for blaming, and by implication shaming, people with MS about lifestyle factors that may impact the long term outcome of their MS. One person said, “stop pushing ‘lifestyle changes’ code for lose weight on people as a fix. It’s insulting and belittling”. In fact, this is incorrect. My dietary recommendations (caloric restriction, intermittent fasting and ketogenic diets) are directed at biohacking and using ketosis as a neuroprotective and pro-remyelinating strategy rather than weight loss. Similarly, exercise (aerobic and HIIT) is about inducing changes within the CNS to promote recovery of function and anti-inflammatory effects in the periphery. The fact that these dietary interventions and exercise can lead to, but not necessarily, weight loss is really not that relevant. Saying this obesity is an issue for pwMS in that that there is a lot of evidence that obesity itself impacts MS outcomes and affects the quality of life of pwMS. In addition, obesity is associated with and causes many comorbidities, which in turn impact MS outcomes (see figure below).
So is obesity a disease or a lifestyle choice? Although this would be a good debate for medical philosophers I am firmly in the camp that at a population level obesity is a metabolic disease that needs to be treated. However, it is up to individuals to choose whether or not they want their obesity treated, in the same way, they have the right to have their MS treated or not.
Some people with MS may not agree with me and hence choose not to have their obesity treated. In these people, obesity is a lifestyle choice and they are presumably well-informed and comfortable with the consequences of being obese. In this situation, who am I to interfere? However, I still feel I have a responsibility to ask the question about the problem?
Because of the sensitive issue of fat-shaming, it is important to open the discussion about weight in a respectful and non-judgmental way. You will be more open to talk about it and seek help if you feel respected. Before asking patients if they wish to discuss their weight, I mention the impact being overweight can have on MS and general health. I usually bundle the weight issue with a discussion about general health and wellbeing. I use the term weight or BMI, which people prefer to the terms such as obesity, obese, fat, excess fat and being overweight. I also cognizant about cultural differences, for example, in certain cultures being overweight is still viewed as a sign of being healthy and/or affluent.
So as a neurologist who manages people with MS should I ignore lifestyle issues such as smoking, alcohol misuse, poor diet, obesity, sedentary behaviour? Maybe this should be left to the GP or family doctor? What does your neurologist do? Another commentator made the point that as I don’t have MS, i.e. have a lived experience of what it is really like to have MS, I shouldn’t expect pwMS to self-manage aspects of their disease such as lifestyle factors. Do you agree?
Please note weight also swings both ways. I have numerous patients who are too thin. Some have eating disorders, others caloric restrict too much to treat their MS, others don’t eat to avoid food coma and others may have a systemic disease associated with loss of weight that needs to be diagnosed and managed. Being too thin is also associated with poor health outcomes. So asking about weight is very relevant to the holistic management of MS.
Please note that over the last 20 years the dogma that obesity is due to ‘too many calories in (overeating) and too few calories out (too little exercise)’ has been debunked. Not all calories are made equal, i.e. not all calorific foods are obesogenic. Obesity is a metabolic or endocrine disorder and there are well-established ways to treat obesity. The corollary is also true, there are well-established ways to become obese. So if you have concerns about your weight, be it that you are underweight or overweight please discuss it with your HCP.
Mendizabal et al. Comorbid disease drives short-term hospitalization outcomes in patients with multiple sclerosis. Neurol Clin Pract . 2020 Jun;10(3):255-264.
Objective: Readmission is used as a quality indicator and is the primary target outcome for disease-modifying therapy (DMT) for multiple sclerosis (MS). However, data on readmissions for patients with MS are limited.
Methods: Using the US Nationwide Readmissions Database, we performed a retrospective cohort study of adults hospitalized for MS in 2014. Primary study outcomes were within 30- and 90-day readmissions. Descriptive analyses compared patient, clinical, and hospital variables readmission status. Multivariable logistic regression models estimated the associations between these variables and readmission.
Results: Of 16,629 individuals meeting the study criteria, most were women (73.7%), aged 35-54 years (48.0%), and Medicare program participants (36.8%). In total, 49.7% of inpatients with MS had 1-2 comorbid medical conditions and 23.7% had 3 or more. Having 3 or more comorbidity conditions associated with increased adjusted odds of the 30-day readmission (adjusted odds ratio [AOR] 1.92, 1.34-2.74). Anemia (AOR 1.62, 1.22-2.14), rheumatoid arthritis/collagen vascular diseases (AOR 2.20, 1.45-3.33), congestive heart failure (AOR 2.43, 1.39-4.24), chronic pulmonary disease (AOR 1.35, 1.02-1.78), diabetes with complications (AOR 2.27, 1.45-3.56), hypertension (AOR 1.25, 1.03-1.53), obesity (AOR 1.35, 1.05-1.73), and renal failure (AOR 1.68, 1.06-2.67) were associated with the 30-day readmission. Medicare insurance and nonroutine discharge were also associated with readmission, whereas patient characteristics (sex, age, and socioeconomic status) were not. The most frequent (26.7%) reason for readmission was multiple sclerosis. Ninety-day analyses produced similar findings.
Conclusions: Comorbid diseases were associated with the readmission for persons with multiple sclerosis. Evaluations of the real-world effectiveness for DMTs in reducing hospitalizations in patients with MS may need to consider comorbid disease burden and management.
Stenberg et al. Bariatric and metabolic surgery in patients with morbid obesity and multiple sclerosis – a nationwide, matched cohort study. Surg Obes Relat Dis. 2021 Jun;17(6):1108-1114.
Background: Despite an association between obesity and multiple sclerosis (MS), very little is known regarding the safety and efficacy outcomes for patients with MS and severe obesity undergoing metabolic surgery.
Objectives: The aim of the present study was to evaluate early complications and efficacy outcomes of metabolic surgery in patients with severe obesity and MS.
Setting: Nationwide, Sweden.
Methods: In this, matched cohort study, 196 patients with an MS diagnosis in the Swedish MS register who were undergoing metabolic surgery (gastric bypass or sleeve gastrectomy) with a registration in the Scandinavian Obesity Surgery Registry (SOReg) were matched 1:10 with a control group without MS diagnosis from the SOReg. A 2-stage matching procedure was used (exact match by surgical method, followed by propensity Score matching, including age, sex, preoperative BMI, surgical center, surgical access, year of surgery, hypertension, diabetes, sleep apnea, and dyslipidemia).
Results: Weight loss at 2 years after surgery was similar for patients with MS and controls (total weight loss 31.6 ± 9.1 versus 31.8 ± 9.2, P = .735). No significant differences were seen in either the overall postoperative complication rate (7.9% versus 7.2%, P = .778), or serious postoperative complications (3.7% versus 2.8%, P = .430). All aspects of health-related quality of life (HRQoL) improved in both groups but less so for the physical aspects of HRQoL in patients with MS.
Conclusion: Metabolic surgery is a safe and efficient treatment for severe obesity in patients with MS, and it leads to subsequent improvements in HRQoL. Further studies addressing the effects of metabolic surgery on MS-related symptoms are needed.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.







